 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 359-363 Case Report Gabapentin and Lamotrigine in Indian Patients of Partial Epilepsy Refractory to Carbamazepine A. Sethi, D. Chandra, V. Puri*, V. Mallika** Departments of Pharmacolgy, Neurology,* and Biochemistry**,
Maulana Azad Medical College and G.B. Pant Hospital,
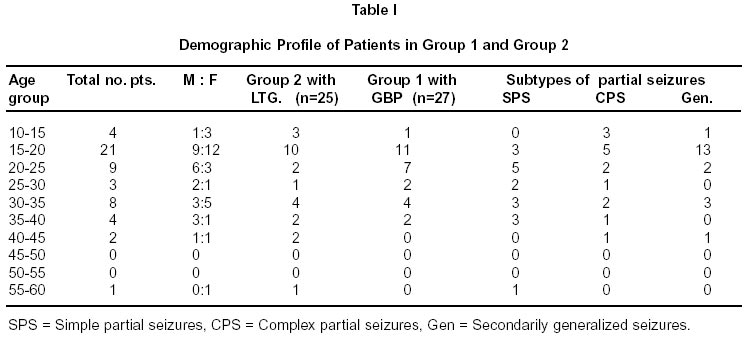
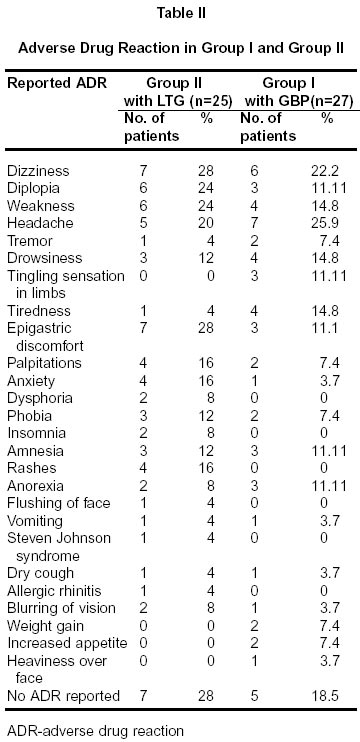
New Delhi - 110 002, India. Accepted for publication : 15th April, 2002. Code Number: ni02100 Summary 52 patients (25 males and 27 females) suffering from refrectory partial seizures, of not more than two years duration and on carbamazepine monotherapy were enrolled in this study. Patients were randomly put on gabapentin (19 males and 8 females) or lamotrigine (6 males and 19 females) as add on therapy. The efficacy of the drugs was assessed by the seizure frequency, pattern of seizures and seizure free interval. The safety was evaluated from the biochemical investigations and the adverse effects observed or reported by the patients during the course of the study. The average frequency of basal partial seizures was 6.26±3.86 and 5.04±2.47 which decreased significantly (p<. 001) after 12 weeks of add on therapy to 1.75±2.16. and 1.68±2.94 in the GBP and LTG group respectively. However, there was no significant difference between the two drugs after 12 weeks of add on therapy. The PCB (primary change in basal seizure frequency) values decreased to -72±34.92 and -76.22±29.68 in the GBP and LTG group respectively. The difference in these two groups was not significant. The responder rate was 77.7% and 92% respectively in GBP and LTG group respectively. GBP was found to be more effective in partial seizures with secondarily generalization while LTG was effective in all subtypes of partial seizures. The abnormal scalp EEG was recorded in 33.3% (9 of 27 patients) in GBP group and 40 %( 10 of 25 patients) in LTG group and it did not revert to normal in 33.3% and 40% of patients in either of groups (GBP/LTG). Minor side effects which were self limiting were noticed in 80% in groups I and 74% were groups II. Key words : Drug treatment, Add on therapy, Partial seizures, Refrectory, Lamotrigine, Carbamazepine, Gabapentin. Introduction The goal of pharmacological therapy in management of epilepsy is complete control of seizures with minimum adverse effects. Monotherapy with conventional antiepileptic agents is effective and well tolerated by a majority of epileptics. However, about 30% patients require more than one drug.1 If the seizures continue despite adequate compliance in proper dosage, there is little evidence that more than 10% of patients with refractory epilepsy will benefit from treatment with two or more drugs.2 Moreover polypharmacy results in a higher incidence of side effects and drug interactions. When a patient becomes refractory to first line drugs, the newer antiepileptic agents i.e. lamotrigine (LTG) and gabapentin (GBP) can be given as add on therapy.3-9 These drugs provide adjunctive therapeutic options and a rational approach to manage such patients. Gabapentin and Lamotrigine are unrelated to standard antiepileptic drugs both in structure as well as mechanism of action; thus ensuring minimum drug-drug interactions. There is a paucity of Indian studies in literature with GBP as adjunctive add on therapies3,4 while there none with LTG.The present study was carried out to assess the efficacy and safety of these newer antiepileptic drug in-patients of partial epilepsy refractory to CBZ. Material and Methods 52 patients (25 males and 27 females) suffering with partial seizures were sampled. All were suffering from epilepsy of not more then 2 years duration and were on CBZ monotherapy. All had at least 4 seizures despite treatment with the maximum tolerated dose of CBZ before being enrolled (baseline) and were considered refractory to CBZ. This corresponded with intractability score of four on Schmidt's scoring system of 0-5.10 Since CBZ has inter individual variations, the maximum clinically tolerated dose was defined as the dose at which neurotoxic adverse effects like nystagmus, diplopia, ataxia etc. appeared in a particular patient. The patients were started randomly on Gabapentin (Group I - 19 males and 8 females), or Lamotrigine (Group II - 6 males and 19 females). Demographic profile of patients in both the groups is shown in Table I. The CBZ drug level was estimated during the baseline (enrolment period) and at 12 weeks of add on therapy using EMIT assay kit. These levels were correlated with the maximum dose of carbamazepine. Patients with structural CNS lesion, hepatic or renal dysfunction or cardiovascular disease, chronic alcoholism, psychiatric illness, pregnant and lactating females, hematological profile with total leucocytes count of less than 3000/mm3 were excluded. All the patients underwent hematological and biochemical investigations i.e. hemoglobin, TLC, DLC, liver and renal profile. All had EEG at enrolment and 12 weeks after add on therapy with either drug (gabapentin or lamotrigine). CT/MR was done in select cases to rule out any structural lesion. In Group I, gabapentin was administered in a dose of 300 mg on day one, followed by 300 mg twice daily on day 2, there after an increment of 300 mg was made daily till seizures were controlled or the toxic effect appeared. The seizures were called as controlled if there was 50 % reduction in the seizures frequency or total control of seizures. In group 2, lamotrigine was added to the treatment regimen in a dose of 50 mg per day for first two weeks followed by 50 mg twice daily for next 2 weeks. Subsequently, at every two weeks interval, increase of 50 to 100 mg per day was made until the similar criteria for seizures control were achieved as for group I. The patients with abnormal EEG in either group I or II had their repeat EEG at every two weeks interval during the study period. The efficacy of the drug was assessed using the seizure frequency, pattern of seizures and seizure free interval.11 The safety was evaluated from the biochemical investigations and the adverse effects observed or reported by the patients during the course of the study. The primary efficacy criteria for efficacy were PCB (percentage change in seizure frequency from baseline i.e. reduction in seizure frequency in percentage at the end of 12 weeks of add on therapy), responder rate (i.e. percentage of patients showing at least 50% reduction in the number of seizures from the baseline) and response ratio (R-ratio) i.e. the difference in number of seizures at baseline and after treatment divided by the total number of seizures (at baseline plus during treatment period). Negative value for PCB and R-ratio indicated reduction in seizures. The Rratio for different subgroups i.e. SPS, CPS and partial seizures with secondarily generalization was also calculated and called secondary efficacy criteria. The responder rate and R ratio was analyzed using chisquare and ANOVA respectively. Results Majority of patients were in the age group of 15-35 years. The average frequency of seizures at baseline was 6.26±3.86 and 5.04±2.47 in the group I and II respectively. This frequency decreased significantly (p<.001) after 12 weeks of add on therapy to 1.75±2.16 and 1.68±2.94. The PCB value was -72±34.92 and -76.22±29.68 in the group I and II, respectively. However, no significant difference was seen in seizure frequency and PCB values in between these two groups after 12 weeks of add on therapy. An inadequate response i.e. less than 50% reduction in number of seizures was observed in 4 out of 27 cases (14.8%) in group I, while, one out of 25 cases (4.0%) in group II, after 12 weeks of add on therapy. The responder rate in group I and group II was 77.7% and 92%, respectively. The responder rate for SPS, CPS and partial seizures with secondarily generalization was 90.9% (10 of 11 cases), 75% (3 of 4 cases), 66.6% (8 of 12 cases) respectively in group I, while corresponding value in group II was 100%(6 of 6 cases), 90.9% (10 of 11 cases), 87.5% (7 of 8 cases) .The seizure free interval in group I increased from basal 9.69±5.32 days to 54.24±34.76 days after treatment while in group II, it increased from basal 7.86±3.85 days to 61.12±33.17 days. But on comparing these groups, the difference was not significant (p <0.2). Abnormal EEG was recorded in 33.3% (9 of 27 patients) in group I and 40% (10 of 25 patients) in group II. But after treatment it was abnormal in three and four patients in group I and II, respectively. Gabapentin was not associated with any significant change in serum concentration of CBZ as recorded at baseline (8.22±2.71mg/l) and after treatment (9.11±3.32mg/l). However, in group II the corresponding value for CBZ serum level was 7.48±2.38mg/l and 9.64±2.60mg/l, respectively with p<0.018. Twenty two patients in group I and 18 in group II, reported side effects during the study period. Most common adverse effects were neurotoxic in both the groups while skin hypersensitivity reactions were observed in group II, only (Table II). Discussion The seizure control was better achieved in the present study with gabapentin as add on therapy as compared to other Indian studies.3,4 In earlier studies, the efficacy of gabapentin was found to be dose related however, in the present study it could not be confirmed.12,13 The drug was well tolerated at all dosages. An increase in number of seizures was observed in one patient who was receiving 2400 mg/d of GBP. While in one large trial with Gabapentin6 the seizure frequency increased in up to 19% of the cases. The seizure frequency at baseline declined to 56% after treatment with gabapentin in comparison to earlier reports of 32% and 57%.7,14 The present study suggested that gabapentin's anticonvulsant action was more pronounced on simple partial seizures and secondarily generalized partial seizures than on complex partial seizures, which is in agreement with study by Crawford et al15 but contrary to US gabapentin group5 which had observed GBP to be more efficacious in complex partial seizures. A significant increase in seizure free interval was seen (p<0.001) after 12 weeks of treatment with gabapentin as reported earlier.3,4,16 Both clinical as well on EEG improvement was seen. A change from the initial clinical presentation of partial seizures to myoclonic jerks or atypical seizures was noted in five patients during treatment, in group I. Gabapentin was not associated with any significant change in serum concentration of CBZ. Such interaction was not expected as this drug does not bind to plasma proteins and nor is an enzyme inducer.17-19 Complete control of seizures was seen in 29. 6 % (8 out of 27 patients) during the study. The common adverse effects reported with Gabapentin were mainly neurotoxic in nature i.e. headache, diplopia, dizziness, drowsiness, weakness etc. But these were mild in nature and none required discontinuation of the drug except in one patient that too due to poor tolerability. This is in agreement with the other reports.5,11,20 In group II, with Lamotrigine as add on therapy, the cent percent seizure control was seen in 44 % (11 out of 25 patients). The mean reduction in the number of seizures at baseline and after treatment was statistically significant (p<0. 001) and similar to those reported by other authors.8,9 A responder rate of 92% was observed with the use of LTG as an adjunctive therapy. This is higher than earlier report of 66.6%.8 All subtypes of partial seizures were controlled effectively although other authors did not observe better results in partial seizures with secondary generalization.21-23 Seizure free interval after treatment with LTG was significantly prolonged, (p<0. 001) similar to the earlier report.8 EEG parameters also showed an improvement with reduction in epileptiform discharges.24,25 The initial clinical presentation of partial seizures changed over to atypical absence and pseudo seizures in two patients each. 74% of patients did not complain of any adverse effects. Two patients terminated the study due to severe adverse reactions i.e. Steven Johnson syndrome (one case) and anxiety neurosis (one case), This patient also had an increase in seizure frequency. Anxiety neurosis as well as increase in seizure frequency has not been reported in the literature with LTG and needs further evaluation with a large study sample. The other adverse effects reported were headache, drowsiness, diplopia, dizziness and dysphoria these have also been reported earlier.25,26 An interaction between LTG and CBZ levels was seen after treatment (p<.01) with LTG. Such interactions have been reported earlier27-29 and attributed towards neurotoxic adverse effects. In the present study, estimation of Lamotrigine as well as CBZ metabolite was not done. Thus the nature of this interaction, whether pharmacokinetic or pharmcodynamic, could not be ascertained. No derangement in laboratory parameters was seen with either drug. The study concludes that GBP as well as LTG are safe with significant antiepileptic activity when added to patients of partial seizures, refractory to CBZ. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02100t2.jpg] [ni02100t1.jpg] |
| |||||||||

{kind=link}
{kind=link}