 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
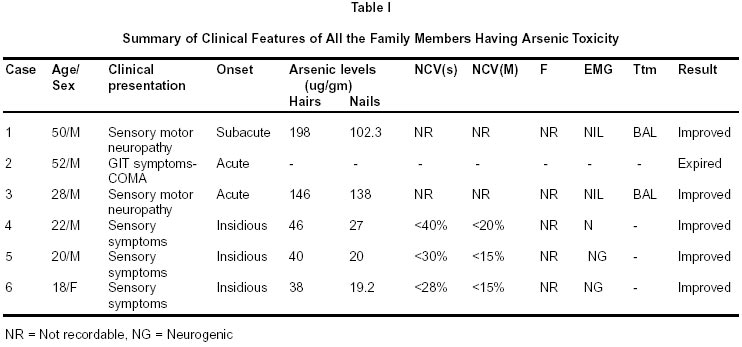
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 364-365 Short Report Arsenic Poisoning in a Family S. Jha, A.K. Dhanuka, M.N. Singh Correspondence to : Dr. S. Jha, Department of Neurology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow - 226 014, India. E-mail : sjha@sgpgi.ac.in Code Number: ni02101 Summary A family of six members is reported, who accidently consumed arsenic, during preparation of indigenous medicine in their home, and developed arsenic poisoning. Key words : Arsenic, Indigenous. Introduction Arsenic has been used in the manufacture of pesticides, rodenticides, paints, pigments and alloys. Ethnic remedies are important source of exposure due to their widspread usage as a component of indigenous medicine.1 BAL has been conventionally used for treatment of chronic arsenic poisoning, but its effectiveness remains doubtful. We report a family of six members with acute and chronic arsenic toxicity. Case Reports A 50 year old lady (case 1) presented with severe vomiting, abdominal colic, and diarrhea, which persisted for 5-6 days. Two weeks later, she developed tingling, numbness, paresthesia and gradually progressive weakness of all four limbs. No cranial nerve, or bladder involvement was present. Examination revealed gross hyperpigmentation of face, arms and upper chest. There was hyperkeratosis of palms. Transverse white lines (Mees) were present in the finger nails. Sensory motor symmetrical, predominantly distal, peripheral neuropathy was present with power around grade 0-1 in all four limbs. The patient was being treated out side as Guillain- Barre-Strohl (LGBS) syndrome. Further interrogation revealed a nearly similar but variable involvement of other family members. Her husband (case 2) and elder son were suffering from severe gastrointestinal problems. The onset was simultaneous in both. While her husband succumed, within 48 hours of illness, inspite of conservative management, the son (case 3) developed severe wasting, weakness and sensory motor flaccid quadriparesis of a similar nature to that of his mother. The two younger sons and one daughter (case 4,5,6) were out of town and returned after the death of their father. They also developed severe diarrhoea, vomiting, abdominal pain along with tingling of fingers and feet within 2-3 weeks. Diagnosis of LGBS was suspected and they were referred. Involvement of all family members raised a doubt of a common toxin. Subsequently all the family members were examined. Mees line and hyperkeratosis was present in all of them, however no neurological deficit was evident. The degree of Mees line suggested a simultaneous exposure. Electrophysiologically severe axonopathy was present in cases 1, 3 while cases 4,5,6 had lesser but significant diminition of amplitudes of motor potentials. Arsenic levels were significantly high in hairs and nails of all (Table I). The elevation was directly proportional to clinical severity of disease and degree of exposure. Collagen profile, CSF, biochemistry and hemogram were normal except for presence of anemia. BAL in a dose 3 mg/kg was given to the two symptomatic individuals (case 1,3) for 14 days. Both of them had mild but significant improvement (grade 1-2 increase in power during hospital stay). At a follow up after 6 months all cases showed significant clinical improvement (Grade 2-3 increase in power in case 1,3). The family was having a business of preparing and manufacturing indigenous medicine for several generations with arsenicals as an important ingredient and the members were consuming a home made vitalizer for health which accidentally got contaminated with arsenicals. Because of relatively less exposure, cases 4,5 and 6 had comparitively less clinical evidence of arsenic toxicity. There is close clinical and electrophysiological resemblance between LGBS and arsenic neuropathy2 as observed in our patients. Rare involvement of cranial nerves and normal CSF in arsenic poisoning helps in differentiating the two. The exact time relationship between exposure to arsenic and appearance of neuropathy is difficult to assess, particularly in Indian subcontinent, where this relationship has been found to be lacking and may vary from days to years,3-5 since chronic arsenic ingestion through indigenous drugs, illicit alcohol or smuggled opium, is the cause. Though BAL has been claimed to be ineffective in aborting or modifying the development of neuropathy especially when given late, it remains the standard treatment in arsenical neuropathy, and has been found to be beneficial provided it is instituted within hours of ingestion.3,6 The interesting aspects of this presentation were involvement of the entire family, exposure of arsenic due to consumption of indigenous medicine, non suspicion of arsenic consumption, proportional clinical and electrophysiological relationship between exposure and presentation and the significant response to BAL in sharp contrast to reports by other authors.5 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02101t1.jpg] |
| |||||||||

{kind=link}