 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
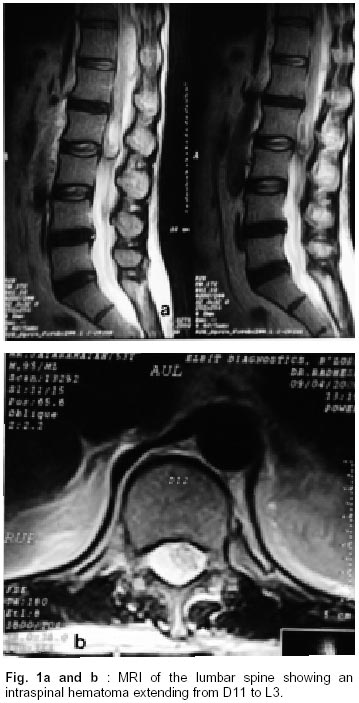
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 367-368 Post Lumbar Puncture Spinal Subarachnoid Hematoma Causing Paraplegia : A Short Report S. Balaji Pai, K.N. Krishna, S. Chandrashekar Correspondence to : Dr. K.N. Krishna, Department of Neurosurgery, M. S. Ramaiah Medical College, Bangalore- 560054, India. Code Number: ni02103 Summary A 53 year old male underwent total excision of a large sphenoidal wing meningioma. Patient was treated with cephalosporins and phenytoin for postoperative meningitis. Three weeks after surgery, a follow up lumbar puncture was done. The patient became paraplegic over a few hours. Imaging of the dorsolumbar spine and other investigations demonstrated a large intraspinal hematoma caused by thrombocytopenia which was probably drug induced. After normalising the platelet count surgical evacuation of the spinal subarachnoid hematoma was done. Relevant literature is reviewed. Key words: Intraspinal, Subarachnoid, Hematoma, Lumbar puncture, Complication. Introduction Intraspinal hematoma is an established though rare complication of lumbar puncture (LP). It occurs most often in patients with bleeding diatheses. Clinical symptomatology may vary from backpain to paraplegia.We report a case of a post lumbar puncture spinal subarachnoid hematoma causing paraplegia in a setting of drug induced thrombocytopenia (DIT). Case Report A 53 year old male underwent a left fronto-temporoparietal craniotomy along with total excision of the left greater sphenoidal wing meningioma. Post operatively he was put on antibiotics (cefotaxime, amikacin and metronidazole), anticonvulsants (phenytoin), steroids and anti-edema measures (mannitol). His immediate post operative blood counts were normal. Repeat CT Scan of the brain confirmed total excision of the tumor with residual edema. Histopathological examination confirmed a transitional meningioma. Patient recovered well and was ambulant by the 7th post operative day. However, he developed fever on the 10th post operative day. Lumbar CSF examination revealed infection (40 cells, 115 mg% protein, 17 mg% sugar, corresponding blood sugar 144 mg%). He was given ceftriaxone 2 gms twice daily and tobramycin 80 mg twice daily for 10 days; following which he became afebrile. A repeat LP done on the 10th day was traumatic. The patient developed paraplegia over next few hours. MRI and CT of the dorsolumbar spine demonstrated a large intraspinal hematoma from D11 to L2 levels with compression of the neural elements (Figs. 1a-b). His bleeding time, clotting time and prothrombin time were all normal. However the platelet count was only 22,000/mm3. Peripheral smear revealed a large number of giant platelets, probably non functional (thrombasthenia) in addition to a low platelet count (thrombocytopenia). High dose methyl prednisolone was started. Eight units of platelet aggregate were transfused and the patient was taken up for surgery. D11 to L3 laminectomy was done. On opening the dura, a large thick subarachnoid hematoma was seen and evacuated. No bleeding source could be identified. Post operatively, he was continued on methyl prednisolone for 48 hours and infused 6 units of platelet aggregate. Tobramycin was continued. Phenytoin however, was changed to phenobarbitone. Patient had an uneventful post operative period during which his platelet count returned to normal. He however, continued to be paraplegic. Repeat CT Scan confirmed complete evacuation of the hematoma without any reaccumulation. Discussion Intraspinal hematoma, though rare is an established complication of lumbar punture.1,2 Post lumbar puncture hematoma may occur in the extradural, subdural or subarachnoid compartments of which the epidural space is the commonest site.1,3,4 Spinal subarachnoid hematoma is extremely uncommon. Domenicucci et al reviewed 106 cases of nontraumatic acute spinal subdural hematoma (SSDH). Most of the cases in their series resulted from bleeding diathesis with or without lumbar puncture.1 Transient paraparesis has been reported after post dural puncture spinal hematoma in a patient receiving ketorolac and as a complication of epidural blood patch.5,6 Clinical presentation of intraspinal hematoma may vary from persistent back pain to frank paraplegia.1-4,7,8 CT and MRI help in identifying the hematoma and its extent.1,2 Patients developing this complication should also be investigated for any existing bleeding disorders.9,10 Early surgical intervention and evacuation is usually indicated. However, in some patients with minimal symptoms conservative treatment may play a role.1,2 Good results may be expected in patients with mild preoperative neurological deficits. Results are poor in patients with subarachnoid hematoma, severe preoperative deficits and in those where surgery has been delayed as in our patient.1,7 Drug induced thrombocytopaenia (DIT) is not rare. A high index of suspicion is the key to diagnosis, especially in the presence of multiple drugs. Patients typically develop purpura and petichae within weeks of introduction of the offending drug, but occasionally within years of starting the drug therapy. Sometimes systemic features like low- grade fever and chills may be seen in early DIT.11 The counts may drop dangerously low (less than 20,000/m3). The bleeding and clotting times, though to a certain extent are influenced by the platelet count, are not truly reflective of the count.12 In our case there was a discrepancy in the counter reading of platelets (20,000/mm3) vis a vis the manual method (65000/mm3). This was attributed to the presence of giant platelets which were probably non-functional. It is difficult to accurately pinpoint the offending drug in our case but ceftriaxone or phenytoin are the most likely culprit. Cephalosporins, apart from causing thrombocytopenia, are described to interfere with platelet function. We feel the platelet count and other coagulation parameters need to be monitored regularly in patients receiving multiple drugs like antibiotics, anticonvulsants and NSAIDs, especially prior to any invasive procedure. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02103f1.jpg] |
| |||||||||

{kind=link}