 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
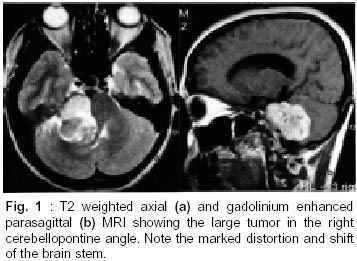
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 369-370 Short Report Facial Myokymia as a Presenting Symptom of Vestibular Schwannoma B.V. Joseph, V. Rajshekhar Correspondence to : Dr. V. Rajshekhar, Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632 004, Tamil Nadu, India. Code Number: ni02104 Summary Facial myokymia is a rare presenting feature of a vestibular schwannoma. We present a 48 year old woman with a large right vestibular schwannoma, who presented with facial myokymia. It is postulated that facial myokymia might be due to a defect in the motor axons of the 7th nerve or due to brain stem compression by the tumor. Key words : Facial myokymia, Vestibular schwannoma, Brain stem. Introduction Facial myokymia (FM) consists of continuous fine rippling activity of all the muscles on one side of the face, due to simultaneous or sequential spontaneous contractions of multiple motor units.1 Electromyogram shows spontaneous asynchronous discharge of adjacent motor units, appearing singly or in doublets or triplets at a rate varying from 30-70 cycles per second.1 It is usually associated with multiple sclerosis2,3 or with intrinsic brainstem tumors.3,4 While hemifacial spasm can be caused by cerebellopontine (CP) angle tumors,5 FM is extremely rare. Case Report A 48 year old housewife presented with decreased hearing of the right ear and involuntary continuous twitching movements of the right side of face for the past 4 years. Over the past two years she developed gait ataxia and headache. On examination she had right sided coarse gaze evoked nystagmus, wasting of temporalis muscle, decreased sensation in V2 and V3 dermatomes, lower motor neurone type of facial nerve involvement, profound sensorineural hearing loss, and decreased palatal sensations. There was continuous abnormal fine rippling movements of the entire right half of face and neck. There were cerebellar signs on the right side. No other deficits were noted. MRI scan showed a large right CP angle tumour measuring 5 x 3 x 4 cms (Fig. 1), enhancing uniformly with contrast, and extending into the internal auditory meatus. There was compression of the brain stem and mild ventricular dilatation. Electromyography showed myokimic discharges at a rate of 30-40/sec, with pseudomyotonic discharges in right frontalis and orbicularis oculi. Facial conductions showed prolonged latencies and decreased amplitude on the right. A right retromastoid suboccipital craniectomy and near total excision of the tumor was done without preservation of the facial nerve.A small 7 mm x 7 mm tumor was left at the VII/VIII nerves root entry zone, as it was adherent to a vessel supplying the brain stem. Postoperatively she had a right lower motor neurone facial palsy. There were no further episodes of myokymia. Postoperative EMG showed fibrillations in the right facial muscles. It was not possible to activate the right facial muscles. No myokymic discharges were seen. Follow-up at 14 months, showed no change in the right lower motor neurone facial palsy. Myokymia was not present. MRI scan showed no residual tumor. Discussion FM is a continuous involuntary rippling movement of unilateral facial muscles. There is continuous flickering from frontalis to platysma, recurring rapidly thereby appearing to pass over the face in rapid undulating waves. Bernhardt reported the earliest case of FM in 1902. Only speculations have been made as to the pathophysiology of FM. Within the brain stem, at supranuclear level, it has been attributed to disruption of inhibitory supranuclear pathways, or isolation of the facial motoneurones. At nuclear level, irritation of the facial motor nucleus has been implicated. At peripheral nerve level, changes in the microenviroment of the intraxial and extraxial course of the 7th nerve have been implicated. Ephaptic transmission, antidromic stimulation with resulant chronic hyperexcitability, and axonal compression and subsequent edema are other suspected contributing factors. A number of conditions can cause FM. It has been described most often with multiple sclerosis2,3 and brain stem masses.3,5 It has also been described in association with Guillain Barre syndrome, unilateral basilar invagination, lymphocytic meningoradiculitis, lymphangitis carcinomatosa, chronic inflammatory polyradiculoneuropathy, following cardiopulmonary arrest, and as a false localizing sign in obstructive hydrocephalus. It has also rarely been described in association with posterior fossa extra axial tumors. To our knowledge, there have been 6 such cases reported so far.3,6-8 A recent review of 1000 cases of vestibular schwannomas revealed that while 0.6% patients had facial spasm, no mention of facial myokymia was made.5 Acknowledgement We would like to thank Dr. Nathaniel Sase for his help with the electrophysiological studies. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02104f1.jpg] |
| |||||||||

{kind=link}