 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
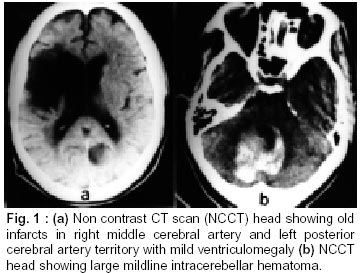
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 373-374 Letter to the Editor Low Molecular Weight Heparin in Management of Intracerebellar Hemorrhage in Patient with Mitral and Aortic Prosthetic Valves A.K. Jain, V. Lal,* Y.P. Sharma, A. Grover Departments of Cardiology and Neurology,* Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India. Code Number: ni02106 The role of low molecular weight heparin in prevention of cardio embolism is yet not proven. We report a case of rnitral and aortic prosthetic valves who had intracranial hemorrhage due to overdose of oral anticoagulation, treated with low molecular weight heparin. Case Report RKC, 50 years male, a known case of rheumatic heart disease (RHD), atrial fibrillation and right middle cerebral artery embolic stroke underwent double valve replacement with - Starr Edwards ball valved prosthesis (Baxter Health Care, Edwards CVS Division, Santa Ana, CA, USA) implanted at Aortic and mitral position in 1990. He was maintained on oral anticoagulants (acenocoumarin 2-4 mg/day) by monitoring INR in range of 2.5-3.0. He continued to do well till 1997 August when he developed tingling sensation on left side of his body and minimal weakness of left lower limb. CT scan revealed a large right temporoparietal infarct (Fig. 1) at an INR of 1.8. No evidence of left atrial thrombus was detected on echocardiography. His acenocoumarin was increased to 6 mg/day to maintain an INR of 3.5-4.5 at a hospital elsewhere. After 10 days, he complained of severe headache, vomiting and dizziness followed by altered sensorium. On admission to this hospital he was drowsy but arousable, pupils were normal sized, normally reacting, dolls eye reflex was preserved and plantars were upgoing. He also had hematuria. His INR at admission was 5.6. A CT scan head revealed a large intracerebellar hemorrhage (Fig. 2). Oral anticoagulant administration was discontinued Inj. K (10 mg) daily along with fresh frozen plasma was given to normalize his coagulation profile. His INR dropped to 1.8 on day 4 of admission, and remained at 1.1-1.3 from day 7 onwards till day 14. His sensorium improved gradually and he could obey verbal commands and move all four limbs. A transthoracic echocardiogram on day 10 and day 14 revealed no evidence of LA clot or valvular thrombosis. Repeat CT scan showed partial resorption of hematoma. After explaining the risks of re-bleeding to the family members he was started on low molecular weight heparin, enoxparin 20 mg subcutaneously per day for 1 week and later 40 mg daily for 3 weeks.A repeat CT scan showed markedly reduced amount of hematoma. After 1 month of therapy with enoxparin, he was discharged on low dose oral anticoagulant acenocoumarin 2 mg daily to maintain an INR between 2.5-3.5. Discussion A patient with prosthetic valves at aortic and mitral positions, in atrial fibrillation and with past history of thrombo embolism, presenting with posterior fossa hemorrhage and grossly deranged coagulation profile poses a difficult management problem. Whereas, intra-cranial hemorrhage is an absolute contraindication to anticoagulant therapy, presence of prosthetic valves mandates obligatory anticoagulant therapy.1 The management of such a clinical problem is not defined in literature. Standard text mentions empirical use of dipyridamole (100/mg four times a day) or aspirin (325 mg daily) or ticlopidine (250 mg twice daily).1 It has been demonstrated that in patients with prosthetic valves undergoing non-cardiac surgery, discontinuing anticoagulants, one to three days prior to surgery and upto one to seven days postoperatively with prothrombin time within 20% of normal range, carries minimal risk of thromboembolism.2 The annual risk of major embolism is adjudged to about 4 per 100 patient years and risk of major embolism is adjudged to be about 4 per 100 patient years and risk of valve thrombosis around 1.7 per 100 patient years. On daily basis this risk works out to be only 0.016%.3 In the presence of intracranial bleed, we withheld all anticoagulants for 2 weeks after INR got normalized, followed clinical status of the patient by CT scan. When the clinical status of this patient improved and CT scan showed signs of resolution of hematoma, low molecular weight heparin in low doses 20 mg S/C once a day was started. LMW heparin has been demonstrated to have low incidence of bleeding complications and thrombocytompenia as compared to conventional heparin.4 Antiplatelet drugs were not considered because of unpredictable response and no proven benefit in preventing thromboembolism in patients with prosthetic valves. It was not considered safe to start low dose of oral anticoagulants because of obvious difficulties in maintaining predictable INR at the initiation of therapy.5 Low molecular weight (LMW) heparin administrations, initially in low doses and with careful monitoring of further CNS bleed, helped in successful discharge of patient on oral anticoagulants. Use of LMW heparin seems to be an alternative option for management of such cases. In conclusion, mechanical prosthetic valve replacement should be carried out with sufficient patient education about the inherent risks of thrombotic potential that it poses. Judicious monitoring of oral anticoagulant therapy with adjustment according to INR is essential. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02106f1.jpg] |
| |||||||||

{kind=link}