 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 380-385 Review Article Cerebrovascular Disease in Type 2 Diabetes Mellitus P.M. Dalal, P.V. Parab Lilavati Hospital and L.K.M.M. Trust Research Centre,
A-791, Bandra Reclamation,
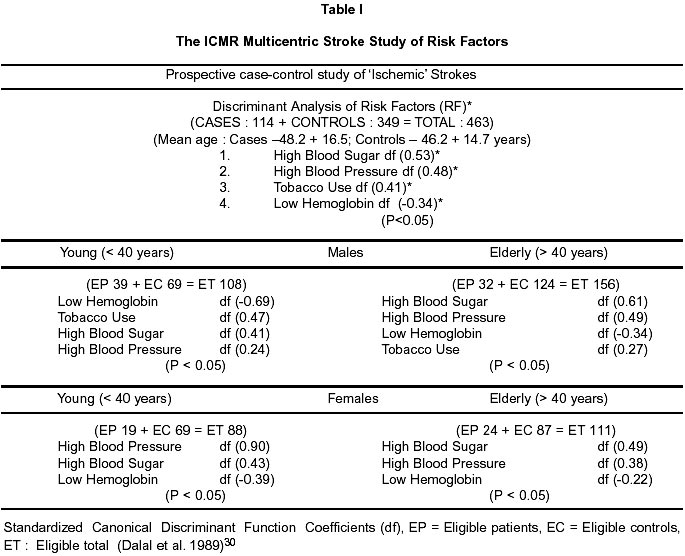
Mumbai - 400 050, India. Accepted for publication : 12th, September 2002. Code Number: ni02111 Summary Incidence of CVD in diabetic men was reported to be twice as that of non-diabetics and almost three times greater in diabetic women in the Framingham Study. It is postulated that excessive glycation and oxidation, endothelial dysfunction and increased platelet aggregation may be responsible for endothelial proliferation and thickening of plasmatic membrane in small blood vessels ('lipohyalinosis') leading to lacunar infarction. Prothrombotic state may precipitate a stroke, however, platelet aggregability, elevated fibrinopeptide A (FPA) and D-dimer were not significantly related to stroke in diabetic mellitus (DM), whereas suppressed fibrinolytic activity was a common finding. Of many unknown factors in pathogenesis, the deficient insulin secretion, resistance to action of insulin at level of 'insulin receptors', changes in counter regulatory hormones (e.g. glucagon, pancreatic polypetides, growth hormone, catecholamines, etc.) and decrease in the hepatic sensitivity to insulin action in suppressing glucose output have received more attention. Hyperosmolar state can simulate stroke syndromes. Early recognition and treatment of risk factors such as hypertension or better glycemic control, correction of hyperlipidemia or obesity in diabetic population are important. In diabetic subjects already showing recurrent transient cerebral ischemic attacks (TIAs) or minor strokes, the benefit of antiplatelet agents or antithrombotic therapy in prevention of major strokes is well established. Ramipril has been found to be effective in reducing stroke risk by 33% in diabetic patinets in HOPE study. Key words : Stroke, Diabetes mellitus, Syndrome X. Introduction There is paucity of literature on the subject of 'stroke' (CVD) in diabetic patients. This is despite the fact that strokes are twice as common in the diabetic population resulting in high morbidity and mortality.1 For India, high prevalence of diabetes mellitus (DM) and impaired glucose tolerance are reported in National Urban Diabetes Survey;2 furthermore, in such subjects there has been high prevalence of carotid intimal medial thickness increasing the risk of stroke.3 Prevalence of Stroke in Diabetic Population The impact of cardiovascular disease was compared in non-diabetics and diabetics in the Framingham cohorts. In the first 20 years of the study, about 6% of women and 8 % of men were diagnosed as diabetics. The incidence of cardiovascular disease in diabetic men was twice that of non-diabetic men and three times in diabetic women as compared to non-diabetic women. Judging from a comparison of standardized coefficients for the regression on incidence of cardiovascular disease as specified risk factors (RFs), there was no indication that the relationship of RFs to the subsequent development of cardiovascular disease was different between diabetics and non-diabetics.4 In the United Kingdom Prospective Diabetes Study (UKPDS), aiming to identify modifiable and nonmodifiable RFs for stroke in type 2 diabetics, 3776 patients aged 25 to 65 years were followed for 7.9 years; 99 of 3776 (2.6%) developed a stroke.5 In a community-based prospective cohort study in Japan, age-adjusted prevalence rate for lacunar infarct was reported to be higher than that of atherothrombotic infarction and cardioembolic strokes in both the sexes.6 Ramchandran et al,7 who examined 3010 subjects (mean age 52 years) attending a diabetic clinic reported cerebrovascular accidents in only 26 cases (0.9%). Retinopathy however was seen in 23.7%, proteinuria in 19.7%, coronary heart disease (CHD) in 11.4% and peripheral vascular disease (PVD) in 4.0% cases. Hypertension was detected in 38% of these subjects. Duration of diabetes had significant correlation with retinopathy, neuropathy and nephropathy CHD and PVD. Likewise, Sridhar reported 186 cases (1.12%) having CVD among 16,384 subjects with type 2 diabetes, in a clinical database spread over a period of 9 years.8 These studies highlight the prevalence of microvascular and macrovascular complications in type 2 diabetes in India.7-8 Pathology and Pathogenesis Diabetes mellitus possibly influences vascular lesions that predispose to brain ischemia and subcortical lacunar infarcts by way of: (i) atherosclerosis of aorta and large extracranial arteries (carotids / vertebrals); (ii) circle of Willis and its leptomeningeal branches, and (iii) degenerative changes such as lipohyalinosis with fibrinoid necrosis as seen microscopically in smaller penetrating vessels.9 In the Japanese population, lacunar infarction has been the most common subtype of cerebral infarction compared to atherothrombotic or cardioembolic infarction.6 However, diabetes is not a RF for a hemorrhagic stroke and the frequency of TIAs (transient ischemic attacks) is not more in diabetics as compared to general population.10 Extracranial vascular disease (carotid stenosis) in diabetics is common but its role in pathogenesis of cerebral ischemic events is still unclear.11-13 For example, in a prospective study of diabetic patients, carotid stenosis (>50 percent) was reported in 8.2 percent as compared with 0.7 percent in age and sex matched controls; 20 percent diabetics with significant carotid stenosis had cerebral ischemic lesions as compared to only 2 percent without significant carotid stenosis. On the other hand, only 28 percent of diabetics with ischemic cerebral episodes had appropriate ipsilateral carotid stenosis, whereas thrombotic lesions in small paramedian penetrating arteries (diameter around 0.5 m µ) resulting in lacunar infarctions appear more common in diabetes mellitus.11-13 Hyperglycemia, impaired carbohydrate tolerance and non-insulin dependent diabetes mellitus (NIDDM) are more prevalent with advancing age. Of many unknown factors in pathogenesis, the deficient insulin secretion, resistance to action of insulin at level of 'insulin receptors', changes in counter regulatory hormones (e.g. glucagon, pancreatic polypeptides, growth hormone, catecholamines, etc) and decrease in the hepatic sensitivity to insulin action in suppressing glucose output have received more attention.14 It is postulated that excessive glycation and oxidation, endothelial dysfunction and increased platelet aggregation may be responsible for endothelial proliferation and thickening of plasmatic membrane in small blood vessels (lipohyalinosis) leading to lacunar infarction.14-15 Prothrombotic states may precipitate a stroke but in studies on prothrombotic states (i.e. platelet aggregability, detection of elevated fibrinopeptide A (FPA) and D-dimer) were not significantly related to stroke in diabetes mellitus whereas suppressed fibrinolytic activity was a common finding.16 Thus, the precise mechanism in pathogenesis of cerebral endothelial damage leading to vascular narrowing and thrombosis remains an enigma. It has also been postulated that high prevalence of stroke mortality in insulin dependent diabetes mellitus (IDDM) subjects may be related to development of hypertension with diabetic nephropathy and disturbances of coagulation-fibrinolytic parameters with increased platelet adhesiveness.16-21 Curiously enough, high morbidity and mortality from strokes is also reported in diabetics after renal transplantation as compared to nondiabetic patients.22 Major factors, which enhance nerve cell injury are an increase in intracellular cytosolic calcium concentration (from failure of ionic pump functions or 'leaks'), changes in Na/K gradients, acidosis, release of glutamate as well as 'excitotoxic' substances, free radicals, and many unknown factors which in turn disrupt the blood brain barrier (BBB) and cell membrane functions, predisposing to cell death.23 Here, energy depletion from ischemic-hypoxia is one of the key events that fails to maintain normal concentrations of cellular adenosine triphosphate (ATP) leading to delay in resynthesis of macromolecular proteins essential for cell structure. Such energy failures also induce proteolysis and lypolysis in addition to production of arachidonic acid, platelet activating factors, free radicals etc. causing further neuronal damage ('ischemic cascade hypothesis').23-24 Thus, severity of cerebral injury is not mere the result of hypoxia from impaired perfusion but end-result of several highly complex 'ischemia-modifying factors'. The role of leukocyteendothelial interaction receptor activation, postischaemic hypo/hyper perfusion damage ('reperfusion injury'), nitric oxide, nerve growth factors and gene expression are under study.23-24 Risk Factors Hyperglycemia or Glucose Intolerance : In Honolulu Heart Program Study,25 7549 Japanese-American men aged 45 to 68 years and free of coronary heart disease and stroke, blood sugar level one hour after a 50 g load was used to classify subjects into four glucose tolerance categories. Incidence of stroke over 22 years was ascertained using comprehensive hospital-based surveillance. Incidence of thromboembolic but not hemorrhagic stroke increased with worsening glucose tolerance category. Compared with the 'low-normal'(glucose > 151 mg/dl) group, subjects in the 'high-normal' (151 to 224 mg/dl), 'asymptomatic high' (>or =225 mg/dl), and 'known diabetes' groups had significantly elevated age - adjusted relative risks of thromboemblic stroke. Insulin-dependent diabetics have increased susceptibility to atherosclerosis in view of increased prevalence of atherogenic RFs (i.e. hypertension, obesity, and abnormal blood lipids).A constellation of metabolic risk factors, termed syndrome X, has also been identified in some type 2 diabetics.26 The main characteristics of syndrome X are hyperinsulinemia and insulin resistance. These results in the secondary features of the syndrome, including hyperglycemia, increased very-low-density lipoprotein cholesterol, decreased HDL cholesterol, and hypertension.26-27 Case-control studies of stroke patients and prospective epidemiological studies have confirmed an independent effect of diabetes on ischemic stroke.28-29 In multicentric prospective case control study on RFs for ischemic strokes in India, high blood sugar as RF was an important finding (Table I).30 In the United Kingdom Prospective Diabetes Study (UKPDS)5 aiming to define significant RFs for stroke, the estimated hazard ratio revealed : (i) advancing age (4.78); (ii) male sex (1.63); (iii) hypertension (2.47) and (iv) atrial fibrillation (8.05) as important RFs. On the other hand, obesity or lack of exercise, poor glycemic control, hyperinsulinemia, dyslipidemia and microalbuminuria were not significantly associated with the stroke.5 Insulin resistance and Ischemic Stroke : Matsumoto et al31 classified 94 stroke cases according to MRI/MRA finding. Insulin resistance was significantly higher (p< 0.001) in subjects having lacunar infarcts (LAC), atherothrombotic infarcts (ATI) and large artery atherothrombotic (LAA) compared to those with normal findings. Multiple logistical regression analysis further showed that insulin resistance was an independent RF in type 2 diabetics. On the other hand, in a recent study32 role of insulin resistance or diabetes mellitus associated with stroke was investigated in 304 Japanese subjects (aged 20-69 years) over 18 years. 28 subjects developed a stroke. In Cox proportional hazard model, hypertension and diabetes, but not insulin resistance, were significant RFs.32 Specific clinical syndromes Many lacunar syndromes have been described in diabetic patients. These are (a) pure motor hemiplegia or (b) pure sensory stroke resulting from lacunar infarcts in basal ganglia, (c) ataxic hemiparesis or (d) clumsy-hand dysarthria syndrome from lacunar lesions in fronto-pontine pathways, and (e) diabetic III nerve palsy or ophthalmoplegia (painful) from vascular lesions in the midbrain. Identical syndromes have been described in hypertensive subjects and it is not uncommon to find both the RFs (hypertension and diabetes mellitus) in the same subjects. In other words, the underlying small vessel disease (microangiopathy with hyalinosis) is identical in diabetic or hypertensive lacunar syndromes. Stroke like syndromes presenting as neurologic deficit with altered sensorium (drowsy state/ semicoma /coma) with or without seizures is not uncommon in diabetic subjects having nonketotic hyperosmolar states. With correction of dehydration and hyperglycemia there is dramatic improvement in neurologic deficit. Thus, 'hyperosmolar states' simulating stroke-syndromes remain strong differential diagnosis. Treatment of Ischemic Cerebrovascular Disease24 Once the diagnosis of ischemic stroke is confirmed by tests like CT Scan, the goal of therapy is to avoid development of brain infarction and, if already present, to prevent its progression or recurrence. Treatment is divided into three phases : Phase I - saving life and speeding recovery; Phase II - rehabilitation to achieve adaptation (physical, occupational, social, etc.) for a gainful employment; Phase III - measures to prevent recurrence of stroke. General and Specific treatment of acute ischemic stroke are described elsewhere.24,33 Stroke Prevention in Diabetics : Early recognition and treatment of RFs such as hypertension or better glycemic control, correction of hyperlipidemia or obesity in diabetic population are important. In subjects having associated myocardial ischemic events, antiplatelet drugs like aspirin have proved beneficial.34,35 In diabetic subjects already showing recurrent cerebral ischemic events (TIAs) or minor strokes, the benefit of antiplatelet agents or antithrombotic therapy in prevention of major strokes is well established.36 Heart Outcomes Prevention Evaluation (HOPE) Study37 : The recent report of the HOPE study in prevention of cardiovascular disease is encouraging. In this placebo-controlled randomised clinical trial, the addition of the angiotensin-converting-enzyme (ACE) 'ramipril' was compared with the current medical regimen of high-risk patients. Here, the substudy of 3577 diabetic patients (of a total population of 9541 participants in the HOPE study) showed a reduction of the primary combined outcome of myocardial infarction, stroke and cardiovascular death by 25% and a reduction of stroke by 33%. This benefit was present even after adjustment for the minor decrease in blood pressure in the ramipril group. There was also a reduction in diabetic complications.37 Hosomi et al (2001) reported retardation of carotid intimal thickening using ACE inhibitor therapy.38 Diabetes Control and Complications Trial (DCCT)39 : DCCT demonstrated that intensive antidiabetic therapy effectively delays the onset of clinically apparent neuropathy in patients with insulin-dependant diabetes. After 5 years of treatment, significant nerve conduction differences were observed between the intensive and conventional treatment group, all favoring better performance (faster sensory and motor conduction velocities and shorter F-wave latencies) in the intensive treatment group. These data suggest that the electrophysiological abnormalities associated with diabetic neuropathy are delayed or prevented by intensive treatment.39 On the other hand, Goldstein and others report that tight control of hypertension in diabetics significantly reduces stroke incidence, whereas tight glycemic control is less effective in stroke-prevention.29 Renal Protection in Type II DM : It is claimed that angiotensin receptor antagonists (e.g. irbesartan), apart from controlling hypertension, has an added benefit of protecting against progressive nephropahty.40 Similar renoprotective benefit is also claimed for losartan.41 Prevention of 'Obesogenic Environment' in Diabetes : The costs of medical care in DM are huge but population screening to identify high-risk subjects (those with impaired glucose tolerance test), and advising them on change of life-style will prove rewarding. For example, 'obesogenic environment' is a driving force leading to weight gain and type 2 diabetes in high-risk subjects. Therefore, an ecological and behavioural approach in prevention of 'obesogenic environment' in community is desirable.42 Conclusion The incidence of ischemic strokes (lacunar type) in diabetic men is twice that of non-diabetic subjects. Early recognition and treatment of RFs such as hypertension, glycemic control, correction of hyperlipidaemia or obesity are important. In diabetic subjects having recurrent cerebral ischemia, benefit of antiplatelet or antithrombotic therapy in prevention of major stroke is well established. The recent favourable report on HOPE study justifies the use of ACE inhibitors (ramipril) in diabetic subjects having brain ischemia. Such therapy may also retard progression of carotid intimal thickening. Acknowledgement We are thankful to Dr. V. R. Bhimani, Executive Vice President and Mr. Prakash B. Mhatre, Director Operations of L.K.M.M.Trust Research Centre and Lilavati Hospital, for permission and unstinted support at all stages. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02111t1.jpg] |
| |||||||||

{kind=link}