 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 386-397 Review Article Management of Congenital Atlanto-Axial Dislocation : Some Lessons Learnt V.K. Jain, S. Behari Department of Neurosurgery,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
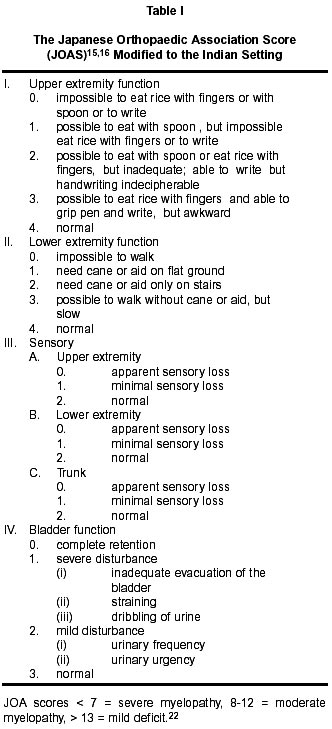
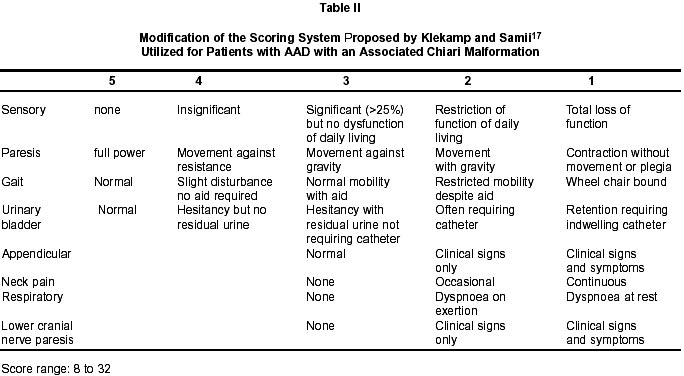
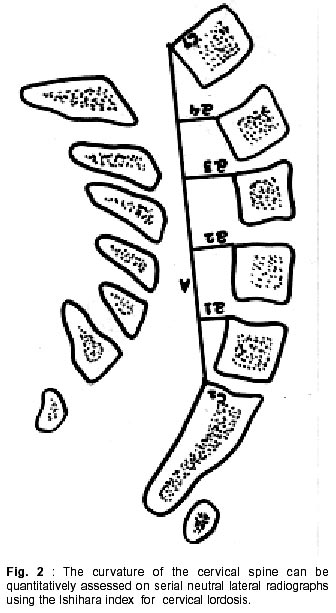
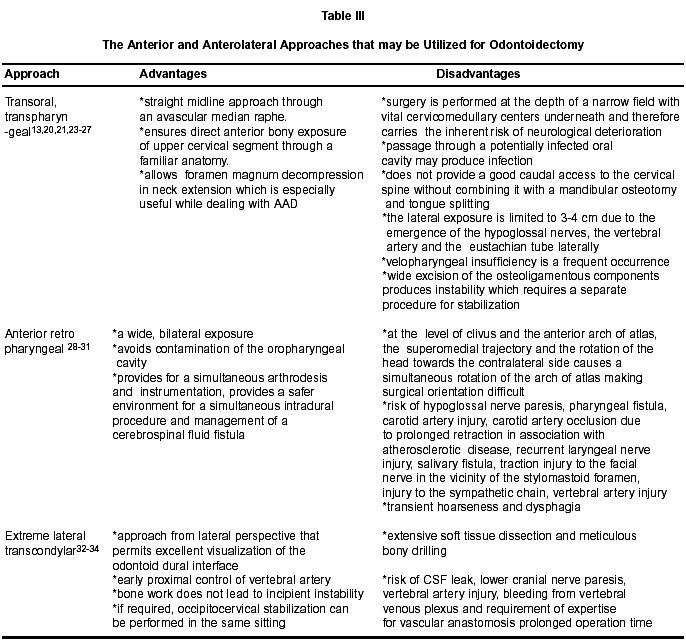
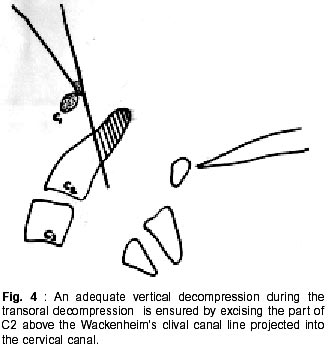
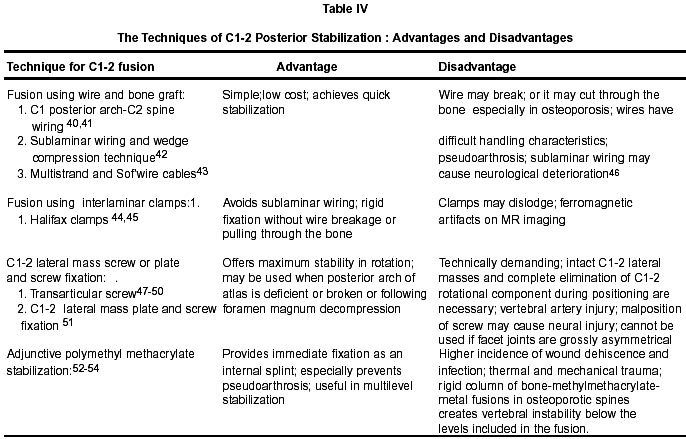
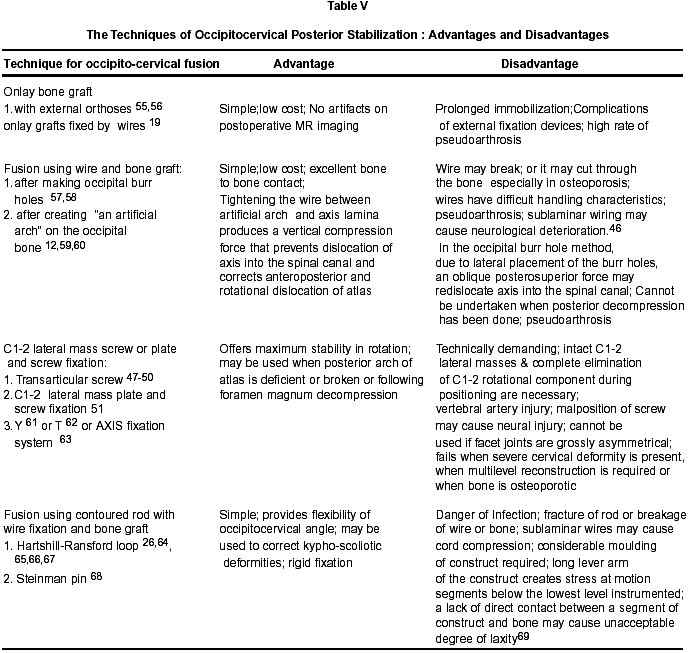
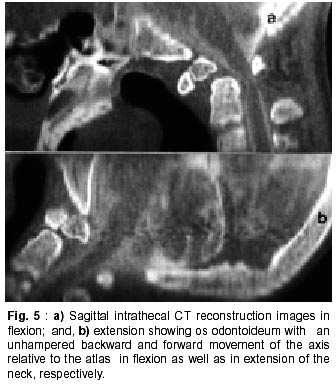
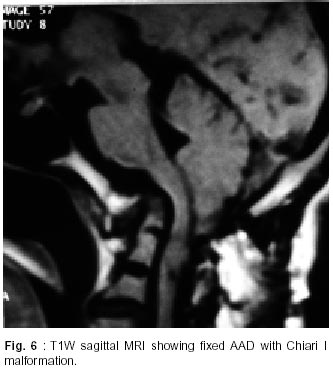
Lucknow - 226 014, India. Accepted for publication : 22nd August, 2002. Code Number: ni02112 Summary Congenital atlantoaxial dislocation (AAD) has a high incidence in India. In these patients, even a minor trauma may precipitate severe morbidity. The management of mobile AAD consists of posterior stabilization. In fixed AAD, the offending compressive element is present anterior to the cervicomedullary junction, which should be generously removed by the transoral approach. In many of these patients, the assimilated posterior arch of atlas or the incurving posterior margin of the foramen magnum or associated Chiari I malformation also adds to the compromise of the canal diameter at the foramen magnum. Thus, in cases of fixed AAD, the hour glass appearance of the spinal canal at the craniovertebral junction should be converted into a funnel shaped appearance which is close to normal. Since these procedures require a generous removal of the osteoligamentous structures, posterior fusion should be done in all cases after decompressive surgery. In this review, the observations that emerged during the management of congenital AAD are presented with a special focus on the assessment scales modified to the Indian settings, hypermobile AAD, rotary C1-2 dislocation, andAAD associated with Chiari I malformation and syringomyelia. Key words : Atlantoaxial dislocation, Transoral surgery, Posterior stabilization. The craniovertebral junction which comprises of the basiocciput, atlas, axis and their supporting ligaments, constitutes the most complex and dynamic region of the cervical spine. The wide range of movements possible at this region makes it vulnerable to injury and instability.1 The complex embryological development of this region also makes it susceptible to a myriad of osseous and soft tissue anomalies.2-10 In this article, we share our experience in the management of congenital atlantoaxial dislocation (AAD) and focus on some of the observations that emerged. Clinical Presentation The classical clinical presentation in these patients include pyramidal signs (weakness and spasticity), stigmata of craniovertebral junction anomalies (short neck, low hairline, facial or hand asymmetry, high arched palate), neck movement restriction and torticollis. The history of transient unconsciousness or sudden neurological deterioration following minor trauma may be elicited irrespective of the presence of mobile or fixed AAD. Functional Evaluation The pre- and postoperative and follow up functional status of our patients was evaluated by a disability grading score11-13 that has four grades viz: Grade I - neurologically intact (present with hyper-reflexia and mild spasticity often with a previous history of neurological deterioration followed by complete improvement), Grade II - independent with minor disability, Grade III - partially dependent on others for their daily needs, and Grade IV - totally dependent. However, for a quantitative evaluation and especially for applying statistical methods, the Japanese orthopaedic association score (JOAS)14-16 modified to the Indian setting is extremely useful (Table I). In patients with AAD with an associated Chiari malformation, a modification of the scoring system proposed by Klekamp and Samii,17 may be utilized for a quantitative assessment of the surgical outcome (Table II). Radiological Evaluation Plain radiographs of the craniovertebral junction (translateral view in neutral position, flexion and extension) are helpful in making the initial diagnosis of AAD; serve as a baseline for the subsequent serial assessment of the extent of distraction and the change in curvature on application of traction; and, can be compared to the postoperative plain radiographs for determining the adequacy of posterior stabilization and bony union. The patients with AAD and a normal posterior arch of atlas with no associated congenital bony anomalies usually have reducible AAD. The reduction may not be evident on plain radiographs of the craniovertebral junction unless sufficient neck extension has been given. Multiplanar dynamic (in flexion and extension) intrathecal contrast CT scan (in axial view and sagittal, coronal and three-dimensional reconstructions) is also undertaken for a threedimensional assessment of the bony configuration of the craniovertebral junction (Figs. 1a and 1b). This has the advantage of adequately delineating the bony abnormalities, the extent of cervicomedullary compression and the presence of Chiari malformation. It can also be compared to a postoperative CT scan where the adequacy of decompression can be assessed by the establishment of the funnel shaped configuration of the cervical canal at foramen magnum as well as by a wide subarachnoid space. At follow up, the formation of a bone block provides a clue to adequate osteosynthesis. The coronal scans reveal facet joint asymmetry and the lateral angulation of odontoid. A preoperative MRI helps to assess soft tissue anomalies, syringomyelia, the extent of cervicomedullary compression and cord changes. However, an MRI at follow up is not possible due to the presence of metallic wires or rods used as implants for posterior stabilization, unless titanium implants are used. A radiological diagnosis of AAD is made when the distance between the anterior arch of the atlas and the odontoid is greater than 3 mm in adults and 4.5 mm in children. In patients with hypoplastic odontoid, the distance between the postero-inferior rim of the anterior arch of atlas and the remaining attached part of the odontoid or the anterior superior edge of the body of axis should be considered.10 However, while diagnosing AAD associated with os odontoideum, Elliot has pointed out that variations existing in the size of the normal odontoid in children should be appreciated and not misinterpreted as odontoid hypoplasia, since the top of the odontoid only reaches the top of the anterior arch of atlas, on an average, by the age of 9 years.18 The associated radiological bony abnormalities that should also be assessed include : basilar invagination occipitalised atlas; bifid or hypoplastic posterior arch of atlas, dens dysplasias facet joint hypoplasia or asymmetry, and, block vertebrae.19 Preoperative Management The AAD may be reducible on extension or may be irreducible.20 In all patients having irreducible AAD, reduction is attempted using Crutchfield's tong traction starting with 7 to 8% of body weight with graded increases to a maximum of 7 Kg over two weeks. Serial lateral cervical radiographs are obtained to monitor the reduction.12,13,21 The preoperative application of the Crutchfield cervical traction improves the neurological status in a majority of patients with fixed AAD due to an increase in the canal diameter caused by both the distraction of the odontoid from the foramen magnum, as well as a change in the curvature of the upper cervical spine so that the tip of the odontoid which is directed posteriorly and kinking the cord, becomes vertical. This change in curvature of the cervical spine can be quantitatively assessed on serial neutral lateral radiographs using the Ishihara index for cervical lordosis (Fig. 2 ).22 Moreover, transoral surgery is facilitated by the distraction of the odontoid from the foramen magnum by the application of traction. In case the patient develops severe neck pain or neurological deterioration or the radiographs of the CV junction show significant distraction at lower disc spaces, then further increase in weight is discontinued even before the maximum weight is reached. The final treatment plan is decided at this stage. Posterior fusion alone is performed in patients with mobile AAD. In patients in whom the deformity is irreducible, with or without basilar invagination, posterior fusion is preceded by ventral decompression (transoral, transpharyngeal)19-21 (Fig. 3a and b). Anesthetic Considerations During intubation, any sudden movements of the neck, especially flexion, should be strictly avoided as they may lead to neurological deterioration. Movements at the atlantoaxial joint may be prevented by placing the cervical collar in position both during intubation and subsequent positioning and by the use of fibreoptic, awake intubation. Initially the patient is anesthetised using a short acting anesthetic, succinylcholine, so that following intubation and positioning, a recovery of the respiratory functions determines that no cord injury has occurred during these procedures. During the transoral procedures, intubation is done by a reinforced endotracheal tube.21 Anterior Decompression The anterior decompression of the odontoid may be performed utilizing different approaches. They have been summarized in Table III.23-34 The usually preferred approach for anterior decompression is through the transpalatal, transpharyngeal route.13,20,21,23-27 In this approach, traction is continued and the patient is placed supine with the head in slightly extended position. The mouth is opened and the tongue retracted using a Boyle-Davis mouth gag. The palate is incised in the midline skirting around the uvula. The anterior arch of the atlas is used as a guide to the midline. The posterior pharyngeal wall is incised in the midline raphe exposing the anterior longitudinal ligament. Then, using the monopolar cautery, the anterior surfaces of the clivus, the C1 anterior arch, odontoid and the body of C2 are exposed upto the C1-2 facet joints on either side. Using a high speed drill, the anterior arch of the atlas and the lower portion of clivus, the odontoid and the C2 body are drilled. The tip of the odontoid is lifted off from the dura, the apical and the alar ligamentous attachments incised and the odontoid removed.25 The posterior longitudinal ligament and the tectorial membrane are also incised exposing the dura. Hemostasis is achieved and the posterior pharyngeal wall and the palate repaired with 2-0 vicryl in two layers using muscle and mucosal sutures. Extent of Excision : An adequate vertical decompression is ensured by excising the part of C2 above the Wackenheim's clival canal line projected into the cervical canal (Fig. 4). Lateral decompression is ensured by drilling the odontoid and axis just beyond the lateral dural margins on either side. This ensures the establishment of the normal funnel shaped dimensions of the upper cervical canal.4,13 Management of Complications of Transoral Surgery : Cerebrospinal fluid leak : In the deeper part of the dens, the cutting drill is changed to a diamond drill which prevents damage to the posterior longitudinal ligament or the dura when the drill penetrates the posterior cortical layer of the dens. The dens is usually resected in its whole width at the base after its initial thinning to separate it totally from the body of the C2. Then the posterior cortex of the dens is pulled up from the posterior longitudinal ligament and dura followed by removal of its apex.13,25A small rent in the dura usually heals by closed lumbar drainage for three days. Larger rents require a fatfascia patch, closed lumbar drainage with acetazolamide administration. Pharyngeal sepsis : As the approach is through a potentially infected oral cavity, there is danger of development of retropharyngeal hematoma due to straying from the midline and dividing the constrictor muscles rather than the midline avascular raphe, and also added risk of infection from the anerobic and candida organisms.11,27,34 This can be been prevented by a strict midline approach, avoiding excessive cautery, meticulous pharyngeal wound closure, obliterating the large retropharyngeal cavity with fat and leaving the last suture at the caudal end of the pharyngeal wound open so that drainage occurs and hematoma formation is prevented.13 In case of wound dehiscence, the wound is allowed to heal by secondary intention as extensive mucosal edema and infection preclude secondary suturing of the wound. The key factors required to promote oral wound healing are adequate nutritional supplementation and oral hygiene. Velopharyngeal insufficiency : Persistant nasal intonation and difficulty in swallowing with nasal reurgitation may be due to abnormal palatal and pharyngeal closure resulting in a scarred palate and pharynx. Palatal wound dehiscence can be corrected by secondary suturing of the palate. Corrective measures include palatal prosthesis or pharyngoplasty.27 Instability : Transoral surgery results in extensive osteoligamentous destruction, precipitating overt or incipient instability, which requires posterior fusion for stabilization.35 After transoral surgery, the anterior landmarks conventionally utilized for the diagnosis of C1-2 instability, including anterior arch of the atlas and odontoid, are excised. The radiological evaluation of the postoperative instability requires assessment of an offset at the C1-2 facet joints on AP view or changes in the spinal-cranial axis, spinolamellar line or the clivus-dens angle ( the obtuse angle between the lines drawn along the clivus and projected into the cervical canal and along the posterior aspect of dens and the body of axis) on dynamic (in flexion and extension) lateral radiographs at the C1-2 joints.36 A three dimensional CT or MRI may be beneficial.37,38 Posterior Stabilization Techniques The transoral surgery and posterior stabilization procedures are usually undertaken under the same anesthesia as advocated by Crockard et al.24 This avoids the danger of injury to the sutured palatal and pharyngeal wounds during reintubation (if a repeat anesthesia is to be given for posterior fusion); the danger of neurological deterioration due to instability at the craniovertebral junction while the patient is awaiting posterior stabilization after transoral surgery; and, the morbidity of prolonged traction required for stability during the interval between the two procedures.4,13 Patient Position and Exposure : After being anesthetised in a supine position on the trolley, the patient is turned prone on the operating table with the head resting on a horse-shoe head-rest. The head is kept in extended position during the exposure. Stability of the head is maintained during surgery by means of a Crutchfield's tong traction. Attention should be directed to the eyes of the patient while the head is resting prone on the horse shoe head rest because direct pressure on the globe may cause blindness from increased intraocular pressure and consequent retinal ischemia.12,13 The suboccipital region, the neck and the lower rib cage are prepared and draped. The skin incision extends from the external occipital protuberance to the spinous process of the C3-4 vertebrae in the midline. The incision is deepened along the midline, avascular ligamentum nuchae, exposing the occipital bone rostrally and identifying the bifid spine of axis. Subperiosteal dissection of the muscles from the posterior arch of the atlas as well as the spine and lamina of the axis and C3 vertebra are carried out up to the facet joints on either side. The exposed bony surfaces are decorticated using drill to promote osteogenesis and bony union with the onlay bone grafts. The vertebral venous plexus around the atlas and the axis may cause troublesome bleeding and may require control by the use of bipolar cautery. The posterior atlantooccipital membrane and the interlaminar ligamentum flavum are removed, exposing the dura underneath. The incurving margins of the foramen magnum may be removed using Kerrison's micropunches and diamond drill.21 The advantages and disadvantages of the posterior stabilization techniques are summarized in Table IV and V.12,19,26,40-69 Fehlings et al68 enumerated the indications for occipitocervical fusion in congenital AAD. These include AAD with assimilated, hypoplastic or bifid posterior arch of atlas; AAD with associated Chiari I malformation requiring posterior decompression; symptomatic basilar invagination or fixed AAD where extensive osteoligamentous excision involves the clivus, anterior arch of atlas, odontoid and body of C2; and, AAD associated with complex kypho-scoliotic deformities of the cervical spine. Postoperative Management : The patients are encouraged early mobilization outfitted with a hard cervical collar.A Minerva jacket or a SOMI brace was required in a few of our patients a) who showed significant mobility at the facet joints during surgery; and b) patients in an extremely debilitated state with flail musculature who underwent reoperations. The adequacy of decompression and fusion is checked by lateral radiographs of the craniovertebral junction and intrathecal contrast CT scan after three to six months. Postoperative adequacy of decompression can be assessed by the establishment of the funnel shaped configuration of the cervical canal at the C1-2 level and by the presence of a wide subarachnoid space both anterior and posterior to the cord. At follow up, the formation of a bone block provides a clue to adequate osteosynthesis. Special Problems Hypermobile AAD due to os odontoideum (Fig. 5 a and b ) : In patients with os odontoideum, there is an unhampered backward and forward movement of the axis relative to the atlas in flexion and in extension of the neck, respectively. Therefore, flexion at the neck causes AAD and canal compromise due to the backward slippage of the axis relative to the ring of the atlas while extension at the neck causes retrolisthesis of the atlas into the spinal canal also compressing the cord. Thus, the atlantoaxial subluxation occurs both anteriorly and posteriorly. Similarly, Fielding et al reported that 8 of their 22 (23%) patients with os odontoideum had both anterior and posterior instability.70 In these patients, there exists a significant risk of neurological deterioration both by flexion and extension of neck during the intubation and patient positioning.71,72 Therefore, intubation and posterior stabilization should be performed with the neck in neutral position, under the guidance of an intraoperative image intensifier, while ensuring that the vertical axis of C2 does not slip anterior to the posterior margin of the anterior arch of atlas during the tightening of the sublaminar wires. In this setting, a C1-2 transarticular screw fixation or a contoured rod placement may also avoid the forward dislocation as well as retrolisthesis of the atlas by maintaining the posterior arch of the atlas and the lamina of C2 in an optimum position with an interposed strut graft. AAD with Chiari type I with syringomyelia (Fig 6) : AAD with Chiari I malformation73,74 compresses vital cervicomedullary centres both from the anterior and posterior aspects. In mobile AAD associated with Chiari I malformation, after ensuring reduction of AAD, a posterior decompression of the rim of foramen magnum along with duraplasty and contoured rod fusion provides adequate foramen magnum diameter. In patients with fixed AAD with Chiari I malformation, with or without basilar invagination, a preoperative cervical traction distracts the odontoid and improves the spinal curvature. Thereafter, a transoral decompression, posterior decompression, duraplasty and contoured rod stabilization is performed. The key to achieving significant neurological improvement is relief of the anterior compression at the foramen magnum either by reduction of AAD in the mobile variety or by transoral decompression in the fixed variety of AAD. The high incidence of assimilated atlas necessitates an occipitocervical rather than a C1-2 stabilization. The C1-2 facet joints in these category of patients are often asymmetrical hence, the contoured rod is preferred over transarticular stabilization techniques. The presence of syringomyelia leads to the persistence of residual neurological deficits despite adequate foramen magnum decompression. However, with an adequate posterior decompression at the foramen magnum, the syringomyelia often shows spontaneous reduction on a long term follow-up. C1-2 rotary subluxation : Certain inherent anatomical features at the C1-2 joints usually resist the rotary dislocation. These include the transverse ligament that retains the dens behind the anterior arch;75 the lateral C1-2 joints that present ovoid, concavo-convex apposing articular surfaces; the alar ligaments that check the excessive lateral rotation to either side. The occurrence of C1-2 rotary subluxation is due to facet dislocation; transverse ligament incompetence leading to AAD; a steep dens-facet angle occurring in children;76 and, an associated asymmetrical facet joints leading to congenital torticollis. The patients usually present with the characteristic 'cocked robin torticollis' with the head tilted to one side and rotated to the opposite side. There is a diminished range of neck movements so that it is possible to increase the deformity but it is not possible to correct it beyond the neutral position.38,77,78 On antero-posterior radiographic projections, the lateral mass of the atlas that has rotated forward appears wider and close to the midline while the opposite lateral mass is narrower and away from the midline. The facet joint spaces on either side appear asymmetrical. The spinous process of the axis is usually tilted in one and rotated in the opposite direction.79 Anteroposterior tomograms may show the two lateral masses in different coronal planes. Fielding77 classified atlantoaxial rotary dislocation into 4 types: Type I : rotary dislocation without anterior shift, Type II : rotary dislocation with an anterior shift of 5 mm or less, Type III : rotary dislocation with an anterior shift of greater than 5 mm, Type IV : rotary dislocation with a posterior shift. CT and MRI may reveal anterolisthesis, widening of facet joint space, a change in orientation of the facets, and 'naked facet sign'. Contiguous facet surfaces can be seen on one parasagittal image and therefore facet subluxation can be diagnosed with relative ease.80-82 Three-dimensional spiral CT images yield high quality surface images, thus, considerably aid in the diagnosis of this entity.38,39 During surgery, a lateral C1-2 mobilization by drilling the joints and instilling intra-articular bone chips renders the atlas completely mobile on the axis. The central landmarks including the posterior tubercle of atlas and the bifid spinous process of axis are identified and aligned. Therefore, when the central braided wire is tightened between the posterior arch of atlas (or the artificial arch in case of an occipitalised atlas) and the lamina of axis is in the midline, both the translational and rotary dislocation get corrected. Notches are made on the superior border of the posterior arch of atlas and along the inferior border of the lamina of axis that anchor the wires and prevent their lateral and medial shifting. Decortication of the facet joints with intrarticular instillation of bone chips further enhances the strength of the posterior stabilization.38 Regrowth of dens after transoral decompression leading to recurrence of myelopathy : Regrowth of dens has been reported to occur in an adult patient, four years after radiologically documented adequate transoral decompression. This caused a recurrence of cervical myelopathy. The symptoms regressed after a repeat transoral surgery.4 Poor respiratory reserve and lack of postoperative neurological improvement : A number of these patients are in an advanced state of myelopathy being dependent on others for even their daily needs. The presence of AAD leads to repetitive cord trauma. Stagnant hypoxia secondary to venous stasis or occlusion of the vertebral and spinal arteries and preexisting microscopic intra-axial abnormalities may also contribute to the neural damage.83,84 The patients who did not show significant neurological recovery at follow-up or those who required a prolonged ventilatory support following surgery, had advanced spastic quadriparesis; compromise of respiratory reserve preoperatively; and/or, hemodynamic instability or bradycardia during surgery.4,13 In debilitated patients with an overt respiratory compromise, often a formal pulmonary function testing may not be possible. In these patients, simple bedside tests that determine a severe compromise in the respiratory status include single breath count and breath holding time. A poor respiratory status is indicated by a breath holding time less than 10 seconds and a single breath count less than 10. However, many of these patients probably have the syndrome of afferent respiratory dysfunction in which, following injury to the reticulospinal tracts in the ventrolateral quadrants of the cervical cord segments one to three, normal facilitatory and modulatory feedback pathways are no longer available to make fine adjustments in the respiratory servo mechanisms.85 Thus, gross responses are handled satisfactorily so that the routine blood gases and vital capacity are deceptively normal and the condition remains undetectable preoperatively but provocative factors like minor trauma, general anesthesia, narcotics and changes in the inspired CO2 mixture may cause respiratory deterioration. Sleep depresses vital functions exacerbating the respiratory depression. A number of cumulative factors like laryngeal edema, pent up larygobronchial secretions, compromise of the diaphragmatic function, weakness of accessory respiratory muscles and increased thoraco-abdominal muscle tone also contribute to the respiratory compromise.4,13 In these patients, an incentive spirometer is used to improve the respiratory reserve. The patients who require a prolonged ventilatory support ranging between two weeks to two months are also given intermittent elective ventilatory support for some time even after being weaned off from the ventilator to prevent a delayed CO2 build-up and respiratory exhaustion. Recurrent laryngeal nerve to phrenic nerve anastomosis, diaphragmatic pacemakers and mobile ventilators have been tried in various centers in order to establish functionally useful ventilation in patients who develop prolonged ventilatory dependence and sleep apnea syndrome. Conclusion A review of the management of congenital AAD based on personal experiences is presented. The surgical management involves radiological assessment to understand the dynamics at the craniovertebral junction, adequate decompression while protecting the underlying cervicomedullary centres; achievement of a firm bony union; and, taking supportive steps to improve nutrition, motor function and respiration. The fact that some patients do not improve to normalcy, despite the advancements points to the challenges that lie ahead in the management of AAD. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02112t5.jpg] [ni02112f5.jpg] [ni02112t3.jpg] [ni02112f2.jpg] [ni02112t4.jpg] [ni02112f3.jpg] [ni02112f6.jpg] [ni02112f4.jpg] [ni02112t2.jpg] [ni02112f1.jpg] [ni02112t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}