 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 398-407 Review Article Tetanus R. Bhatia, S. Prabhakar, V.K. Grover* Departments of Neurology and Anesthesia*,
Postgraduate Institute of Medical Education and Research,
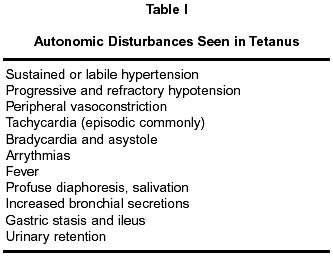
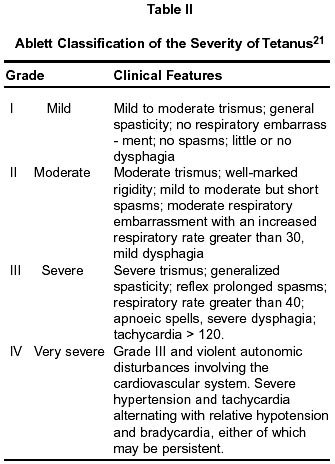
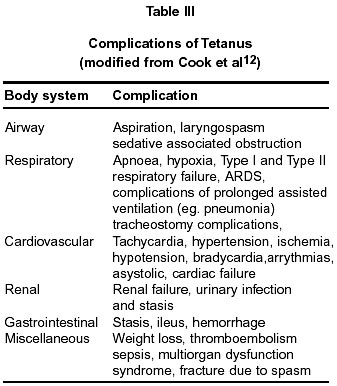
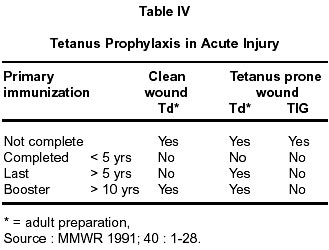
Chandigarh - 160 012, India. Accepted for publication : 20th August, 2002. Code Number: ni02113 Summary Tetanus is a potentially life threatening disease affecting nearly 50,000 to 1 million people world wide every year. Four major clinical forms of tetanus are described i.e. generalized, cephalic, localized and neonatal. Neonatal tetanus is particularly common in developing countries, due to unhygienic child birth practices, social taboos and improper immunization of pregnant mothers. Management of this disorder involves a team approach and aims at eradicating focus of infection, neutralizing the toxin, controlling spasms and dysautonomia and providing adequate ventilatory and supportive care. Metronidazole may be the preferred antibiotic although penicillin is still used frequently. Adequate wound debridement is necessary to prevent spore germination. Spasms are usually managed by sedatives like diazepam and neuromuscular blocking agents. Magnesium sulphate is an attractive substitute and may be tried if ventilatory facilities are unavailable. Use of baclofen is potentially advantageous but cannot be routinely prescribed. Dysautonomia is difficult to manage and requires therapy with benzodiazepines, morphine, magnesium sulphate, adrenergic blockers and recently tried baclofen therapy. Supportive care including ventilatory assistance are highly essential for successful outcome of the patients. It is imperative that complications are diagnosed early and managed appropriately. Immunization is extremely effective and is the key to prevention. Adequate steps and measures should be taken to increase awareness of this potentially preventable disease. Key words : Tetanus, Spasms, Lock jaw. Tetanus is a potentially fatal disease manifesting itself as painful spasms, autonomic instability and respiratory compromise, caused by 'tetanospasmin' a potent neurotoxin liberated by the organism 'clostridium tetani'. Despite the availability of a highly effective vaccine, nearly 1 million cases of tetanus occur worldwide every year.1 Majority of the tetanus related deaths occur in Africa and South-east Asia, and the disease remains endemic in many countries worldwide.2 The present review deals with a brief overview of the disease, available treatment options and methods of prevention. Brief History and Epidemiology The clinical descriptions of tetanus are available in records from antiquity (5th Century BC). In the year 1884, Nicolaier produced tetanus in animals by injecting them with soil specimens. Kitasato isolated the organism in 1889 from a human tetanus victim and reported neutralization of toxin by specific antibodies. Tetanus toxoid was described by Descombey in 1924 and was effectively used during the world war II. The global incidence of tetanus is about 18 cases per 100,000 population per year, with case fatality ranging between 20 and 50%. In places like USA, the incidence of this disease has dramatically reduced over years whereas in developing countries it is still observed frequently. At least 40-50% of deaths occur in neonates, especially due to unhygienic conditions during birth and social practices like smearing cow dung or ghee (clarified butter) on umbilical stump.3 During a tetanus surveillance from USA between 1995-1997, 60% of cases were between 20-59 years of age, whereas in prior reports, population above 60 years was more commonly affected.4 Punctures, lacerations, and abrasions accounted for 64% of reported cases. The higher risk in elderly is possibly related to a decline in protective levels of antibodies with ageing and therefore a booster dose of vaccination is recommended every 10 years to ensure protection.5 Almost all reported cases of tetanus are in patients who either have never been vaccinated, or who completed a primary series, but have not had a booster in the preceding ten years. Although the incidence of tetanus is grossly underreported in India, it has shown a downward trend due to the national immunization programme.6 Considering the seriousness of this disorder, adequate wound hygiene and thorough immunization practices are warranted to prevent the occurrence of this potentially fatal disease. The Organism Clostridium tetani is a gram positive, obligately anerobe, spore forming bacillus, which give it a characteristic drumstick or a tennis racket appearance. The organism is widely distributed in soil and in intestine of horses, sheep, cattle, dogs, cats, rats, chickens and nearly 10% of humans.7 The spores can also be found on skin surfaces and in contaminated heroin. In agricultural areas like ours, a significant number of human adults may harbor the organism. Although the vegetative forms of this organism are sensitive to heat and oxygen, the spores are especially resistant to heat, usual antiseptics and chemical agents but are destroyed by autoclaving at 120°C for 15 minutes or boiling for atleast 4 hours. The vegetative form produces 'tetanospasmin', a potent neurotoxin which is responsible for the clinical manifestations and ranks second to the botulinum toxin as the most potent microbial toxin known.7 Pathogenesis Under anaerobic conditions, spores present around the wound germinate. This leads to production of two known toxins : 'tetanospasmin' and 'tetanolysin', which are disseminated by blood and lymphatics to several sites within the nervous system. Tetanolysin has a uncertain role and major clinical effects of the disease are secondary to the action of tetanospasmin. The toxin is produced as a polypeptide but undergoes post-translational cleavage into two di-sulfide linked fragments, the light (L) and heavy (H) chains.2 The H chain mediates attachment to gangliosides in peripheral nerves and subsequently the toxin is internalized and moves to the CNS by retrograde axonal transport and trans-synaptic spread. Once inside the CNS, the 'L' chain mediated cleavage of synaptobrevin (an essential component of synaptic vessels needed for fusion and release of neurotransmitters) prevents presynaptic release of inhibitory neurotransmitter g-aminobutyric acid (GABA) and glycine, causing sustained excitatory discharge of disinhibited a-motor neurons and muscle spasms of tetanus. The toxin exerts its effects on the spinal cord, brain stem, peripheral nerves, neuromuscular junctions, and directly on muscles.2 The rapidity of incubation and onset correlates with severity of the disease. Recovery involves synthesis of new presynaptic components and their transport to distal axon,8 accounting for the delay of 2-3 weeks before clinical improvement begins.1 Clinical Manifestations Four clinical forms of this disease are recognized depending upon the extent and location of neurons involved.1 The incubation period ranges from 7-14 days, although periods as short as one day to as long as several months have been reported. This may be related to the amount of toxin present at the site of wound and immunization status of the patient. The time of onset is defined as the period between the onset of symptoms and start of spasms. This helps in prognostication and correlates with the severity of disease,7 with shorter periods associated with a severer disease form. Generalized tetanus : This represents the commonest form of the disease and is characterized by increased muscle tone and generalized spasms. Usually, the first symptom is difficulty in opening jaw, due to increased tone of the masseters (trismus or lock jaw). Subsequently, there is a spread to other body parts. Dysphagia, stiffness and pain in neck, shoulder and back muscles appears. Rigidity of abdomen and facial grimacing, popularly known as 'risus sardonicus' (ironical smile), may appear due to facial muscle contraction. Eventually, there is appearance of generalized muscle spasms, occurring spontaneously or due to minor stimuli such as noise, touch, or nursing procedures.2 The spasms are immensely painful and may lead to respiratory compromise necessitating respiratory support. Spasms may complicate the picture by causing compressive fractures of the spine, rupture of muscles, rhabdomyolysis and renal failure. These are maximum during the first two weeks of illness and decrease thereafter in frequency and intensity. Autonomic instability is of major concern, and usually develops few days after the onset of the disease (Table I). There may be labile or sustained hypertension, tachycardia, arrhythmias, hyperpyrexia, profuse sweating, peripheral vasoconstriction, hypotension and bradycardia.9,10 Dysarrhythmia and myocardial infarction are the most common fatal events.11 Possible pathogenesis involves sympathetic nervous system disinhibition and elevated catecholamine levels.1,9-12 Severe hypertension and tachycardia may alternate with profound hypotension, bradycardia or recurrent cardiac arrest.12 These alterations predominantly result from rapid alterations in systemic vascular resistance rather than cardiac filling or performance.13,14 Other autonomic effects include profuse salivation, increased bronchial secretions, gastric stasis, ileus and high output renal failure.12 Localised tetanus : This is a relatively uncommon and benign form of the disease process in which patients have persistent contraction of muscles in same anatomic area as the injury preceding the tetanus. Local tetanus might generalize over time but overall mortality is about 1%. However, in a recent retrospective study of localized tetanus in 45 patients, 7 (16%) died and 5 (11%) had sequelae.15 The most important indicator for poor prognosis was the progression to secondary generalization (27%). Cephalic tetanus : This involves cranial nerves and has an overall incidence of 6%.16,17 It commonly results from middle ear infections and head injuries.17 Facial muscles are most commonly affected, followed by 6th, 3rd, 4th and 12th cranial nerves in the order of frequency. Trismus may be present but usually follows other cranial nerve deficits in 42% of patients.16 Although, overall mortality described is high (15-30%), many cases with a milder disease have been reported from India.18 Neonatal tetanus : This form of tetanus still has a high incidence and mortality in the developing countries with an estimated 500,000 deaths per year.19 A hospital based study showed application of `ghee' (clarified butter) on the umbilical stump as a potential risk factor for tetanus in neonates.3 The common age of onset is between 5 and 15 days following birth. Common presenting complaints are rigidity, spasms, failure to suck, trismus, fever and seizures. Due to lack of inhibiting influences from higher centers in newborns, the anterior horn cells react more violently, resulting in more spasms.6 Overall mortality is around 70% and most patients with severe disease die. Improved immunization coverage, clean delivery practices and cord care , and changes in social taboos are necessary to reduce morbidity and mortality of neonatal tetanus.19 Many prognostic grading systems (Phillips, Dakar, Udwadia) are reported. Phillips score20 and Ablett (Table II) are outlined. The system reported by Ablett is simple, useful and most widely used.21 Overall mortality is variable and is dependent upon immune status, age of the patient and availability of facilities for management. In developing countries, mortality rates exceed 50% with respiratory failure being the major cause of mortality and morbidity.12 Mortality is highest for those older than 60 years and in neonates. Complications in tetanus may result from the disease itself or are related to management. These have been outlined in table III. Diagnosis and differential diagnosis The diagnosis of tetanus is primarily clinical. History of injury, or presence of a wound aids in strengthening the diagnosis. In patients, where the portal of entry is not evident, a careful search for signs of parentral drug abuse, otitis media, instrumentation, injections or minor surgical procedures should be inquired.6 No definite laboratory abnormalities are present and the CSF is usually normal. Electromyography during tetanic spasms shows continuous discharges of normal motor unit potentials similar to normal forceful voluntary muscle contraction. However, the silent period that occurs 50 to 100 ms after reflex contraction normally is lost. This pause is mediated by recurrent inhibition of Renshaw cells which is inhibited by the tetanus toxin. Peripheral nervous system involvement is supported by the observations of muscle fatigue, distal paresis, muscular atrophy, decreased reflexes and electrophysiological studies.6 Prabhakar et al showed evidence of a predominantly sensory neuropathy by electrophysiological and histological studies.22 Differential diagnosis of tetanus includes: i) painful conditions of lower jaw, ii) Bell's palsy, iii) meningitis, iv) drug induced dystonia and dyskinesia, v) rabies, vi) globus hystericus, vii) strychnine poisoning viii) tetany, ix) acute abdomen, x) stiffman's syndrome etc. Appropriate history and physical examination can differentiate most of them. Apte and Karnad described a bedside `spatula test' to aid in diagnosis with a sensitivity of 94% and specificity of 100%.23 A spatula is carefully inserted into the pharynx. If patient gags and expels the spatula, the test is negative for tetanus. If however, the patient bites the spatula because of the reflex spasm of masseter, the test is considered positive. The test may not hold the same value and sensitivity in areas with low incidence of tetanus because of the presence of other commoner etiologies Management Management of tetanus patients involves a team approach. The approach depends upon resources, personnel, and expertise at one's command.24 Symptomatic management, early recognition of complications, careful monitoring for dysautonomia and respiratory assistance are the anchors for successful outcome of any patient. Presence of intensive care units have changed the overall outcome from a dismal to a more hopeful one. In our country, where intensive unit care cannot be available at all hospitals, general medical and nursing care administered conscientiously by those familiar with the disease can reduce mortality from 30% to 15%.24 The costs of intensive care are tremendous and clearly unrealistic in most parts of the world where tetanus is a major problem. The clinical course of tetanus is often unpredictable and patients need close monitoring throughout the illness. Ventilatory assistance, respiratory failure, renal dysfunction, autonomic imbalance and complications of prolonged critical illness like nosocomial infections, sepsis, thromboembolism and gastrointestinal hemorrhage need special attention.2 The defined goals of treatment include the following : a) halting production of toxin within the wound, b) neutralization of unbound toxin, c) control of muscle spasms, d) management of autonomic instability, e) supportive therapy, f) management of complications, g) prevention. a) Halting the production of toxin (i) Wound management : Debridement of a wound is important to eradicate spores and change conditions for germination, thereby preventing further elaboration and absorption of the neurotoxin. Wound characteristics strongly correlate with the development of tetanus. Recent linear wounds with sharp edges that are well vascularised and not obviously infected are usually non-tetanus prone. All other wounds are considered potentially predisposed, especially those that have resulted from blunt trauma, bites and are obviously contaminated.1 (ii) Antibiotic therapy : Penicillin and metronidazole are the two major drugs used routinely. Penicillin still remains a standard therapy in many parts of the world, although metronidazole seems to be replacing it and is being considered as a drug of choice by many.1,2,12,25 Metronidazole has a better safety profile, better tissue penetrability and negligible CNS excitability (penicillin can cause seizures at high doses). It can also be given rectally which minimizes and reduces frequency of spasms, which otherwise would be precipitated by an I/V or I/M medication. Ahmadsyah and Salim26 showed improvement in mortality with use of metronidazole butYen et al27 and Singhi et al28 did not report the same benefit. However, where available, metronidazole should be the preferred antibiotic. The usual dose of penicillin is 100,000 - 200,000 IU/kg/day given intravenously or intramuscularly. Metronidazole is used at a dose of 500 mg every 6 hours intravenously or per orally and 400 mg rectally every 6 hours, for 7-10 days. (b) Neutralization of the unbound toxin This is achieved through passive immunization with either human or equine tetanus immunoglobulin. This should be undertaken as early as possible since the toxin becomes inaccessible once it is bound to the nerve terminus. Human tetanus immunoglobulin (HTIG) is the preferred form because of lack of immunogenecity and a longer half life of 24-31 days. The equine formulation has a high likelihood of anaphylactic reactions and has a half life of only 2 days. The usual dose of equine preparation is 500- 1000 IU/kg given intravenously or intramuscularly. The dose of HTIG is 5000-8000 IU intramuscularly. Local infiltration around the wound is not recommended presently. Usual dose for prophylaxis is 1500-3000 IU of equine and 250-500 IU of human preparation.2 The blood concentration of antitoxin for protection against tetanus is 0.1 IU/ml. Intrathecal therapy with antitoxin has been tried in the past, but a meta-analysis of the same showed no obvious benefit of such a therapy.29 (c) Control of muscle spasms Spasms in tetanus are potentially life threatening, for they impair respiratory function, produce exhaustion and often lead to aspiration of gastric contents. Many drugs have been used for the effective control of spasms in tetanus patients. Sedation has been the mainstay in the past and is still used as the primary therapy in most of the centres for its easy availability. However, use of muscle relaxants is frequent in intensive units and sedation is used as a adjunct to management. Sedatives : Benzodiazepines have been traditionally used for control of spasms. Diazepam is the most commonly used drug of this class, and is usually the first drug to be used in the initial phase of the illness. The doses used have been variable, depending upon the patients clinical condition and response. The average dose used as an adjunct to muscle relaxants is 10-30 mg 6-8 hrly, and is usually the starting dose even when used solely. Doses upto 120 mg/kg/day have also been used.30 Respiratory depression and prolonged sedation are major problems at high doses and appropriate ventilatory assistance is imperative. Midazolam has been used with beneficial effects but is expensive and needs more respiratory assistance. However, its relative short duration of action and early reversability of sedation are distinct advantages over diazepam therapy.31,32 It is imperative to titrate doses gradually for the risk of sedation, respiratory depression and accumulation of metabolites.33 The drug should be tapered gradually to avoid withdrawl reactions. Propofol, a general anesthetic, has been used with benefit in control of spasms and rigidity,34 and has been corroborated with neurophysiological studies.12 Adverse effects include hypotension, bradycardia, pain at injection site, hypertriglyceridemia, pancreatic dysfunction and need for mechanical ventilation.33 Prolonged use of propofol (>48 hrs) has been associated with lactic acidosis, bradycardia and lipemia in children and is therefore not recommended for pediatric use.33 It is strongly recommended that propofol infusion bottles and tubing should be hanging for no more than 12 hours and solution transferred from main vial be discarded after 6 hours for the risk of bacterial overgrowth and nosocomial infections. (ii) Neuromuscular blocking agents : The use of these drugs becomes imminent, when sedation produces no benefit. However, intubation with positive pressure ventilation is mandatory. Commonly, pancuronium has been widely used for its lesser cost. However, potential risk of worsening autonomic dysfunction is present because of its effects on catecholamine uptake. Vecuronium is considered the drug of choice because of negligible cardiovascular effects, but is short acting and cost is a limiting factor. It has a potential risk of accumulation in presence of renal failure. Recuronium is highly safe but expensive. Monitoring of patients on muscle relaxant therapy is difficult and it is important that doses of relaxants be spaced out after 2 weeks and usually stopped after three weeks to prevent complications and adverse effects on long term use. Prolonged recovery from paralysis is thought to be related to accumulation of drugs or their metabolites. Acute quadriplegic myopathy syndrome or AQMS is common when steroids are taken concomitantly and reports of this dysfunction with use of neuromuscular blocking drugs alone is uncommon.35 It usually presents as a acute paresis with myonecrosis, increased CPK and abnormal EMG. Other potential hazards with use of these drugs is muscle contractures, atrophy and risk of venous thrombosis or embolic events related to immobility. Pancuronium may be a safe option to start with if no cardiovascular dysfunction is present. In presence of severe hepatic or renal disease, cisatracuronium or atracuronium may be used.36 Eye care is essential and concomitant use of steroids is discouraged. (iii) Magnesium sulfate : Role of magnesium sulfate in the management of tetanus has been postulated by many authors.37,38 Blake treated two patients of tetanus with intrathecal magnesium sulfate, as early as 1906.39 Magnesium physiologically antagonizes calcium and there is a correlation between depression of neuromuscular transmission and serum magnesium concentrations.37 Use of magnesium sulfate has the added advantage of controlling dysautonomia, where it has been more commonly used. Considering the ease of administration, availability of experience in managing patients with eclampsia, and avoidance of sedation and mechanical ventilation, the drug seems definitely advantageous in management of tetanus related spasms. However, more trials and experience with the use of this drug is required. It is usually given as a loading dose of 5 gm over 20 minutes followed by a regular infusion at a rate of 2 gm/hour. Abolition of patellar reflex is taken as the endpoint and evidence of hypocalcemia is judged by positive Chvostek's and Trousseau's signs. The drug is best avoided in the presence of severe renal failure. (iv) Baclofen : Baclofen, a physiological GABA agonist has been used in few small studies for effective control of tetanic spasms.40-43 The drug inhibits mono and polysynaptic medullary reflexes, resulting in a antispastic action.43 It has been shown to stimulate postsynaptic GABA b receptors, thereby restoring physiological inhibition of a motor neurons. High dose intrathecal baclofen has been used for the treatment of tetanus induced contractures and spasms, thereby limiting the need for general anesthesia and intubation in afflicted patients.40 The preferred route of administration is intrathecal for the drug is 600 times more potent at a much lesser dose compared to the oral route. The half life of this drug is between 0.9 to 5 hours. The largest series published is by Engrad et al43 who have reported 14 patients treated with this regimen, of which it was effective in twelve. However, baclofen has a narrow therapeutic range and a large interindividual pharmacodynamic variability. The cost of therapy and need for surgical expertise (in case infusion pump is required), are major deterrents for its use. The dose is variable and on an average is about 1000 mcg in adults below 55 years, 500 mcg below 16 years of age and 800 mcg for adults above 55 years. Intermittent boluses may be given initially at an interval of 10-20 hours depending upon the response of the patient or it may be given by a continuous infusion if frequent doses are necessary. Caution is desired in patients with severe dysautonomia and when spasticity is used to obtain increased function. (v) Dantrolene : It is a directly acting muscle relaxant mediating its action through inhibition of calcium release by sarcoplasmic reticulum and thereby directly affecting excitation contraction coupling. It has been used in isolated cases in the past for managing tetanic spasms and has the major benefit of not requiring artificial ventilation. However, the drug is expensive and cannot be recommended for routine use. (d) Management of dysautonomia Dysautonomia is a significant problem in patients with tetanus and drug therapy is aimed at stabilizing the cardiovascular system while preserving compensatory mechanisms, so as to avoid sudden collapse and death. Many drugs have been used with this aim but none is devoid of potential problems. Drugs have been used with the aim to produce adrenergic blockade or to prevent release of catecholamines and thereby suppress autonomic hyperactivity.44,45 Following drugs have been used with the aim to treat dysautonomia. Sedatives : These drugs were used in the past to improve early dysautonomia, and benzodiazepenes especially diazepam is still used with this aim. Since this drug has a wide margin of safety, is cheap and commonly available, can be given through all routes, and has muscle relaxant and anticonvulsant properties, its use in the initial part of illness is justified. However, at high doses, it itself is a respiratory depressant and produces excessive sedation which necessitates ventilatory assistance. Phenothiazines, like chlorpromazine were used in view of its a-adrenergic blocking action and some complex effects which may be due to additional blockade of neuronal uptake of amines. Since high doses of this drug may itself increase catecholamine levels, it is preferable to avoid doses above 200 mg/day. It causes a centrally mediated fall in BP, but despite theoretical advantages, it provides unsatisfactory control of cardiovascular disturbances.9 Morphine is another drug used for management of dysautonomia. It has excellent sedative properties and minimal effect on cardiovascular performance.2 It reduces mean arterial pressure, heart rate and systemic vascular resistance while having minimal effect on the cardiac output.45 However, high doses are required and a continuous infusion is appropriate. The drug possibly causes CNS depression of sympathetic outflow, although multiple sites of action might exist. Intrathecal or epidural morphine might seem efficacious, but overall results through these routes have not been as satisfactory.9 The usual dose is 5-30 mg given as a infusion over 30 minutes every 2-8 hours. Most patients would respond to a dose of 0.1 mg/kg every 4-6 hours. Daily doses range between 20- 180 mg/kg. Epidural anesthesia is another regime which seems promising. Bhagwanjee et al46 described their observations on 11 patients treated with epidural bupivacaine and sufentanil using midazolam as an adjunct with encouraging results. Further trials are needed to generalize its use. Adrenergic blockers : Labetolol has been frequently used to treat adrenergic overactivity for it produces dual adrenergic blockade,47 although the b-blocking effect is more significant. However, concerns about myocardial damage and cardiac arrest were raised in view of unopossed release of catecholamines, and impaired peripheral vasodilation.2 Propranolol was one of the earliest drugs used in its class, but fell out of use because of reports of fatal cardiovascular failure and irreversible cardiac arrest in the patients treated. Esmolol, a short aching b blocker, has been useful in suppressing crisis but does not prevent catecholamine release. Clonidine, a centrally acting sympatholytic agent has been used with beneficial effects and has the added advantage of being an anxiolytic and sedative.48 Post ganglionic and alpha adrenergic blocking drugs like guanethidine and phentolamine have been used in the past but fell out of use due to disadvantages of hypotension, tachyphylaxis and rebound hypertension. Magnesium sulfate : It is a promising drug and has been used in management of spasms as well as autonomic overactivity.37,49,50 Magnesium causes presynaptic neuromuscular blockade, blocks release of catecholamines, reduces receptor sensitivity to released catecholamines, and has anticonvulsant and vasodilator properties.2 In view of these properties, this drug has been extensively used in the management of eclampsia worldwide. However, the drug has been associated with sedation, impairment of tidal volume, cough and need for ventilation at high doses.2,49 Tacheostomy is mandatory and availability of ventilatory support is imperative.2 The doses used have already been outlined in the management of tetanic spasms. Although quite promising, the exact role of this drug needs more evaluation for recommendation in routine use. Intrathecal baclofen : As outlined in the management of spasms, this drug has also been used with success in managing dysautonomia. Although it has been proposed as a agent of benefit in tropical milieu for the reduction in need for artificial ventilation,40 in all reports a significant number of patients had developed coma and respiratory depression necessitating ventilation.2 Probably, interindividual dose variability is high and therefore dose modifications and guidelines for its use are needed. Another potential problem and concern in tetanic patients is the risk of infection through spinal intervention. Supportive Management General supportive care plays a major role in the outcome of these patients. In a critically ill patient, the complication of prolonged hospital stay and instrumentation are sufficient enough to delay the process of recovery. It is imperative to realize the necessity of adequate nursing care and regular vigil in management. These patients are predisposed to nosocomial infection, bed sores, tracheal stenosis and GI hemorrhage.2 Securing the airway is primary and helps in preventing aspiration and assisting ventilation. Initially, endotracheal intubation is justified, but considering that the recovery is likely to be slow and need for mechanical ventilation may be long, tracheostomy is a much better option. This also avoids undue stimulation of upper airway and prevents spasms and respiratory complications from aspiration and hypoventilation. Percutaneous tracheostomy is preferred to open surgical techniques for it reduces blood loss and long term sequelae.2 Tracheostomy site should be regularly cleaned using maximum sterility. Assisted ventilation is often used in tetanus patients, especially where spasms impair respiration and all attempts should be made to detect patients with incipient hypoxia and respiratory failure. We advocate controlled mandatory ventilation in the initial stage of disease. As stabilization occurs, the patient is shifted to pressure support and PEEP modes. In the later stages, modes allowing spontaneous ventilation (SIMV, CPAP) are preferred. It is suggested that weaving be done as early as possible to minimize the problems associated with prolonged paralysis and neuromuscular blockade. Chest physiotherapy and regular tracheal suction are essential to prevent atelectasis, lobar collapse and pneumonia.2 Secretions and salivations may be difficult to manage, and can be minimized by using nebulization with ipratropium. Other supportive measures like meticulous mouth care, nursing the patient in 150-300 sitting position, regular washing of hands and keeping I/V access sites clean are small, but significant steps in patient management. Nutritional requirements of these patients are high and weight loss is a common finding, making nutrition management a significant factor. This should be commenced as early as possible through a nasogastric tube or where facilities allow, by percutaneous endoscopic gastrostomy, because it prevents undue stimulation and reduces spasms. Prevention and Immunization Hygienic practices during child birth, prompt and adequate wound care and enforced immunization schedules are key to prevent this disease. In fact, considering the efficacy, availability and cost of this vaccine, it is sad that still so many deaths occur every year in developing countries. Emphasis on the preventive aspects of this disease and awareness of the seriousness of the illness but easy ways of prevention need to be stressed upon. Changes in social taboos and adoption of hygienic practices during child birth are likely to reduce the high incidence of neonatal tetanus present in our country and around the world. Vaccination is highly safe and efficacious. Active immunization should be instituted in all partially immunized and unimmunized adults as well as those recovering from tetanus. In patients with tetanus, passive immunization in forms of tetanus immunoglobulin is usually combined with active vaccination, so called active - passive immunization.2 This adds to a long term hormonal and cellular immunity. The prescribed schedule for patients depending upon the nature of wound is given in table IV. It is important that different sites are chosen for immunoglobulin and toxoid injection to prevent interaction. If used together, no more than 1000 IU of human or 5000 IU of equine antitoxin should be administered for the risk of neutralizing the effect of toxoid. Tetanus vaccination is instituted in the form of a toxoid, which consists of a formaldehyle treated toxin standardized for potency in animal tests. Two types of toxoid are available ; adsorbed (aluminium salt precipitated) and fluid toxoid. The former is preferred because of a better and longer lasting response. Tetanus toxoid is available as a single antigen preparation, combined with diphtheria vaccine as pediatric DT or adult Td, and with both diphtheria and pertussis vaccine as DTaP. Children younger than 7 years should receive either DTaP or pediatric DT and adults and children above 7 years should receive Td formulation. Single antigen tetanus toxoid is not recommended. In children, 3 doses of DPT vaccine are given at an interval of 4-8 weeks, starting at 6 weeks of age, followed by booster at 18 months. The second booster (DT) is given at 5-6 years and third upto 10 years. The initial series for adults involves 3 doses. The first and second doses are given 4-8 weeks apart and the third is given 6 months after the second. Booster doses are required every 10 years to maintain protective antitoxin titers. Tetanus does not confer immunity because of the small toxin amount needed to produce illness. The minimum protective level of antitoxin is 0.01 IU/ml, which is usually achieved in all recipients of vaccine who have completed primary series of properly spaced doses of tetanus toxoid. Immunization of all pregnant women is an important step in preventing neonatal tetanus. Two or three doses of tetanus toxoid are administered during pregnancy with last dose administered one month before delivery. Local adverse reactions to the injection include erythema, induration and pain at injection site which are usually self limiting. Fever and other systemic symptoms are uncommon. Other reactions include exaggerated local (arthrus like) reaction seen commonly in adults who have received frequent doses, generalized urticaria, anaphylaxis and neurological complications like neuropathy, Guillaine-Barre syndrome and brachial neuritis have also been reported.51 The vaccine is usually contraindicated in patients who have had a severe allergic reaction in the past with the toxoid and caution is advocated for its use in presence of a moderate to severe concomitant illness. Research for better and simpler approach for tetanus vaccination is hoped for the future. Single dose vaccination using microencapsulation techniques may be desirable, but needs more refinement.52 Mortality and Outcome Overall mortality of this condition is variable and varies between 25-50% for generalized tetanus and is as high as 85-90% for neonatal tetanus, with respiratory failure and cardiac dysautonomia being the chief causes of death. The outcome is poor in neonates, elderly and in patients with short incubation periods and short interval between onset of symptoms and the first spasm. In USA, a mortality of 11% was recorded between 1995 and 1997.4 In our institute, a mortality of 18% was recorded53 and in a recent study from Malaysia, the mortality was again 18%.54 It was observed that mortality is highest in grade III tetanus and those with a nosocomial infection.53 The course of tetanus extends over 4-6 weeks with long periods of ventilatory support. Increased tone and minor spasms may persist for months but recovery is generally complete. Conclusion Tetanus remains a problem of immense concern worldwide, with a high mortality in the elderly and neonatal population. Management of tetanus with its attendant complications are challenges to the physician. Although symptomatic therapy has improved over time no definite consensus on adequate treatment is available. Prevention is the chief priority and it is absolutely essential that people are educated about this potentially serious but extremely preventable disorder, for this is the only step towards global eradication. Probably, a better understanding of the disease process and its effects on nervous tissue will aid in effective management of cases. We look towards the future with hope of seeing a tetanus free planet. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02113t2.jpg] [ni02113t1.jpg] [ni02113t4.jpg] [ni02113t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}