 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
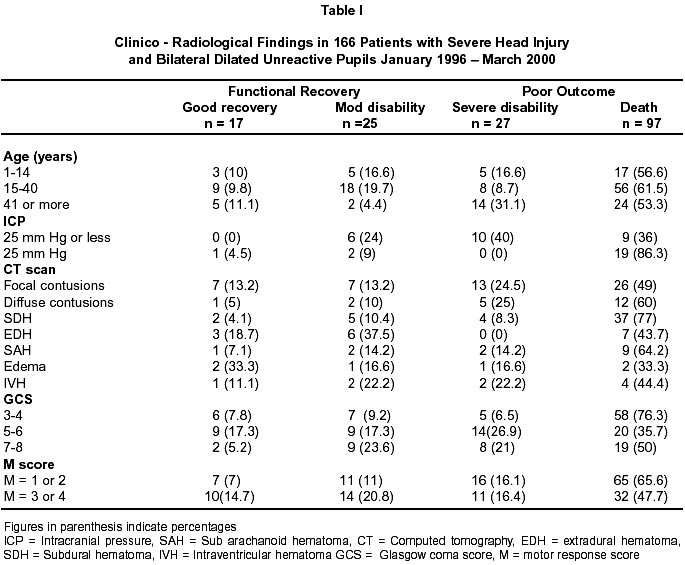
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 430-435 Long Term Outcome in Patients with Severe Head Injury and Bilateral Fixed Dilated Pupils J. Sousa, R.R. Sharma, S.J. Pawar, A. Mahapatra, S.D. Lad Department of Neurosurgery,
Khoula Hospital,
Muscat 116, Sultanate of Oman. Accepted for publication : 15th December, 2001. Code Number: ni02117 Summary Patients with severe head injury with bilateral dilated unreactive pupils are considered to have a grave prognosis. Hence proper planning and aggressive management becomes mandatory for achieving good results.We present the outcome of consecutive 166 patients with severe head injury, admitted between January 1996 and December 2000 and analysed retrospectively. All the patients had an initial GCS of 8 or less and post resuscitation bilateral dilated unreactive pupils. Our aim was to analyze the long term outcome in these patients and identify the other significant prognostic factors. Of the 166 patients, 42 (25.30%) had a functional outcome (good recovery in 10.24%, moderate disability in 15.06%), and 124 (74.69%) had a poor outcome (death in 58.43% and severe disability in 16.26% of cases). There were 45 patients with polytrauma and 24 of these patients (53.33%) succumbed to the injuries. Obliteration of the basal cisterns and contusion were the common CT scan findings. Factors adversely affecting the survival included age of the patient, polytrauma with shock, initial GCS of 3 or 4, and compression of the basal cisterns on the initial CT scans. At follow up, most of the patients with a functional outcome showed a significant improvement in their motor function but continued to have neuro-behavioral and cognitive deficits. Key words : Pupil, Unreactive, Dilated, Severe head injury, Outcome. Introduction Generally, patients with severe head injury, presenting with bilateral dilated unreactive pupils are considered to have a grave prognosis.1-3 Such a presentation suggests the possibility of a significant brain injury. Although, many studies have identified the prognostic factors in severe head injuries, few studies have focussed on the severe head injury patients with bilateral dilated unreactive pupils in predicting the long term outcome.4-10 This study was planned to determine the outcome in this group of patients and also to identify other prognostic factors, to help plan further line of management. Material and Methods Clinical information was obtained through retrospective analysis of the 166 patients with bilateral fixed dilated pupils, admitted at the National Neurosurgical Center, Khoula Hospital, Sultanate of Oman, over 5 year period from January 1996 through to December 2000. The patients were followed up regularly at the neurosurgical out patient clinic to determine the ultimate outcome. Follow-up ranged from 6-40 months (mean 24 months). During the study period, 1245 patients were admitted in the neuro intensive care unit with severe head injury (Glasgow Coma Score 8 or less). 166 patients were admitted with post resuscitation bilateral dilated and unreactive pupils. There were 148 males and 18 females. Demographically, 136 patients were adults and 30 were children (upto the age of 14 years). All the patients had a pupillary size of 4 mm or more. Patients having direct ocular trauma or indirect optic nerve injury were excluded from the study. Prior to the elective ventilation, post resuscitation, the glasgow coma score (GCS)11 was carefully recorded in these patients. CT scans were performed in all cases, as soon as possible. ICP monitoring was carried out in 62 patients as per our ICP protocol. Both intraventricular and intraparenchymal methods were used depending on the suitability. Patients having ICP of > 20 mm Hg, received mannitol regularly. In patients with intraventricular catheter, CSF drainage was regularly used as a modality to reduce ICP, when ICP was > 20 mm of Hg. Patients with significant focal mass lesions were subjected to surgical evacuation, provided, they were not in irreversible shock or diagnosed as brain stem death. Duration of ventilation and ICP monitoring was reviewed on daily basis and continued as per the need. Blood gases, cerebral perfusion pressure (CPP) and electrolytes were monitored carefully. Patients requiring ventilation longer than 2 weeks, often required tracheostomy. Outcome was assessed following the criterion of glasgow outcome scale (GOS).12 Patients were followed in out patient clinic on regular basis. Functional outcome was defined as a good clinical outcome or a moderate disability as described by Andrews and Pitts, in 1991.1 Results a) Modes of Injury : 51 patients (30.7%) out of the total 166 were pedestrians involved in road accidents, 82 (49.4%) were passengers in cars involved in high speed road accidents. Twenty-nine patients (17.4%) had a fall from a height and in 4 patients (2.4%) the injuries were due to a fall from a camel. The latter is unique to this region, where camel racing is a common sport, with children acting as the camel jockeys. b) CT scan findings and Outcome : Among the focal mass lesions, a single small brain contusion was the commonest CT scan finding recorded in 49 patients (31.9 %). A large cerebral contusion was seen in 4 cases. This was followed by an acute subdural hematoma (SDH) in 48 patients (28.9 %). The SDH was small in 38 cases and large in 10 cases. 16 (9.6%) patients had an extradural hematoma (EDH). In only 9 cases EDH was significant enough to be evacuated. Other CT scan findings included, scattered small contusions in 20 patients (12%) and traumatic sub arachanoid hemorrhage (TSAH) in 14 cases (8.4%). Six patients (3.6%) had generalized brain swelling. Partial or complete obliteration of basal cistern was recorded in 132 cases (80%). Overall 124 patients had a poor outcome, among them 118 (95.1%) had obliteration of the basal cistern on the CT scans, whereas a group of 42 patients with a functional outcome only 14 cases (33%) had obliteration of basal cisterns. c) GCS and Outcome : Of the 76 patients with initial GCS score of 3 or 4, 63 patients (82.8%) had a poor outcome (p<0.05). Of the 54 patients with an initial GCS of 3, 49 patients expired (90.7%). A preparalysis extensor response (M 2 response) was associated with a functional outcome in only 18 of 99 patients (18.1 %). Level of significance in outcome in patients with M1 and M2 response was high ( p<0.01), while a flexor response (M=3 or 4) was associated with a functional outcome in 24 of the 67 patients (35.8%) (p< 0.01). ICP and outcome : Intracranial pressure (ICP) monitoring was done in 62 cases. In the pediatric age group 70% of the patients with a mean ICP of > 15 mm Hg, had a poor outcome. In the adult group, 19 of the 25 patients (76%) with a mean ICP pressure of 25 mm Hg or less had a poor outcome, while 19 of the 22 patients (86.36%) with a mean ICP of more than 25 mm Hg had a poor outcome. Surgery : Nine cases of EDH were operated upon and 6 (66.6%) survived with a functional outcome. Out of 10 patients with acute subdural hematoma who were operated upon, only one (10%) survived with severe disabilities. Of the 4 operated patients with contusions who were operated, only one (25%) survived with severe disabilities. Overall Outcome : Of the 166 patients, 69 patients (41.2%) survived, 42 (25.3%) with a good functional outcome. In the pediatric patients (1-14 years), 13 of the 30 patients (43.3%) were discharged, 8 (26.6%) with a functional outcome. Of the 45 patients with associated polytrauma, 24 (53.3%) succumbed to their injuries. None of the 20 patients with polytrauma and hypotension survived. Among the patients who expired, the mean hospital stay was 6.94 days, whereas, the patients who survived had a mean hospital stay of 57.23 days. Follow up : The survivors were followed up for 6-40 months. Of the 69 patients who survived, 9 were lost to follow up. Of the 25 patients with moderate disability, the motor weakness improved significantly in 20 patients (80 %) in the first year post trauma, but did not show much improvement thereafter, inspite of regular, intensive physiotherapy. However, neurobehavioral and cognitive deficits persisted in most of the patients. Unfortunately, 17 of the 27 patients (62.9%) discharged with severe disabilities remained so, even after 16-30 months following their discharge. Discussion Adoption of the glasgow coma scale (GCS) and the glasgow outcome score (GOS) have provided practical methods for assessment of the severity and the outcome in patients with severe head injury (GCS 8 or less). Aggressive management of these patients with elective ventilation has meant that a neuro surgeon has to rely on the pupillary reflexes, CT scan findings and ICP monitoring to guide his further decisions. While the pre- paralysis GCS score tends to reflects the effects of the primary impact, rather than the secondary compression, recovery from initial low GCS scores are well known.2 Thus, the paralyzed patients may actually have a better or worse GCS score than the initial recorded score. It is interesting to note that in severe head injuries the post resuscitation GCS score has been reported to be the most predictive of neurobehavioral outcome at one year, while the 24 hour GCS score has been shown to be most predictive of cognitive recovery at 2 years.3,4 While it was predicted that aggressive management of severe head injury would decrease mortality, but increase the number of vegetative patients, studies have shown that percentage of patients with functional outcome actually increases without significantly increasing the percentage of severe disabled patients.5 Many prognostic factors following head injury have been widely recognized.5-9 However, very few studies have focussed exclusively on the outcome of patients with dilated unreactive pupils, thus giving a special significance to our study.2 Miller et al,10 reported associated polytrauma in 49% of cases in their series. Forty five patients (27.1%) in our series also had associated polytrauma, with a mortality of 53.3%. Neufiled et al13 reported a high mortality of 83% in patients with severe head injury in shock, while Andrews et al1 had poor outcome in 95.55% of severe head injured patients with hypotension and cardiac arrest. A single episode of hypotension has been reported to cause an 85% increase in mortality.14 Mechanical trauma has been shown to increase the vulnerability of the brain to ischemia for a period that may last for upto 24 hours.15 The resulting ischemia, if present, occurs in the first few hours following the trauma.18 It has also been shown that the cerebral autoregulatory function and CO2 vascular reactivity was impaired to absent in the injured brain.6,17,18 Hence, it is not suprising that polytrauma patients with hypotension have been reported to be associated with a poor outcome.13 Children with polytrauma are especially vulnerable to hypotension, which is compounded by their need of comparatively higher cerebral blood flow and oxygen requirements.19 Brain stem blood flow of less than 40 ml / 100 g / min, in patients with bilateral unreactive pupils is associated with a poor outcome.20 However, Bouma et al21 showed that, these patients in addition to a decreased brain stem blood flow also demonstrated a global cerebral hypoperfusion (cerebral blood flow of 18 ml / 100 gm / min or less). Brainstem blood flow on xenon CT studies revealed no correlation with brain stem dysfunctions.21,22 Interestingly, Sakas et al2 in 1995 reported that 17.5% of patients in their series had bilateral unresponsive pupils and localizing motor response. In our series, 33 patients (5.3%) had a flexor motor response (M 4 respnnse) and 60.6% of these patients (20 out of 33) had a functional outcome. While lack of pupillary responsiveness and motor abnormalities are thought to reflect brain stem ischemia, frequent involvement of the third nerve nuclei in the brain stem suggests its higher vulnerability to ischemia than the corticospinal pathway.2 As demonstrated in our study, effacement of basal cisterns on CT scan has also been reported to be associated with a poor prognosis.2,23-25 This may reflect the fact that compressed or absent basal cisterns have been shown to be an important indicator of raised ICP.23 Marmarou et al26 reported that besides the age, motor score and pupillary responses the ICP measurement at admission were the factors most likely to affect the outcome. ICP recording was also shown to be superior to the cerebral perfusion pressure (CPP) in predicting the outcome.26 It should, however, be noted that the ICP may be normal for the first 24 hours and may rise as late as 3 days following the trauma.27 It is interesting to note that the hyperventilation probably has its most deleterious effect during the first 24 hours after severe head injury, when the cerebral blood flow is typically at its lowest.13,22 An initial middle cerebral artery flow velocity of less than 28 cm/sec on transcranial doppler (TCD) has been reported to be associated with a poor outcome.28 Although, patients with bilateral dilated unreactive pupils are reported to have a poor prognosis,10,11 functional outcome in patients with unreactive pupils has been reported in 3.5%,1 to 25%2 patients. In the present series, the mortality rate was 58.4% with a functional outcome in 25.3 % of patients. Functional outcome has been shown to be better in the younger age group.6,29-31 In the present study, 29.6% of the patients between the ages of 15-40 years had a functional outcome, followed by 26.6 % of patients below 15 years of age, as compared to the patients of > 40 years of age, who had functional outcome of cases. This may be a reflection of the mechanism of injury, associated injuries and the functional reserve in these patients to sustain the stress. Patients with decerebrate rigidity are reported to have a poor outcome.6,32 Bricolo et al reported a good outcome only in 16% cases.32 In our study, 81.8% patients with an extensor response had a poor outcome with 18.2% achieved a good functional outcome. Various biochemical parameters like serum catecholamine levels,33 serum glucose levels,34 coagulation parameters.35 CK-BB (Creatinine Kinase BB)36 have also been studied to predict the outcome in patients with severe head injury. Timing of the outcome assessment is also very important, since premature assessment of outcome may underestimate the recovery.37 Hence, it is also important that a persistent vegetative state should not be diagnosed, till the end of the first year after the trauma.38 Usually, a patient classified as functional outcome will have achieved this status by the first 6 months.37 Heiden et al reported that 68% of the patients classified as severe disability at 1 month, had improved to the category of moderate disability or a good recovery at 6 months and 72% had achieved this status at 1 year. Interestingly, while the initial linguistic impairment is largely due to a dominant hemisphere injury, long term recovery of language function is most dependent on the duration of the coma.39 Conclusion Patients with severe head injury and unreactive dilated pupils, should be aggressively managed. Age, shock on admission, and obliteration of basal cistern on the initial CT scan determine the survival. The best predictors of a favourable outcome in severe head injury patients with fixed dilated pupils include young age, Glasgow coma scale above 4/15, stable vital signs in the normal ranges, and the presence of basal cisterns and absence of midbrain shift on the initial CT scans. The unreliable predictors were initial ICP recordings, the presence of DAI or SAH on the initial CT scans. Surprisingly, ICP failed to predict the outcome. GCS of 3 (M = 1 or 2) is associated with a poor outcome, Patients with bilateral fixed dilated pupils and EDH should be operated upon as a significant number of these patients in our study had a functional outcome. Reference
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02117t1.jpg] |
| |||||||||

{kind=link}