 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
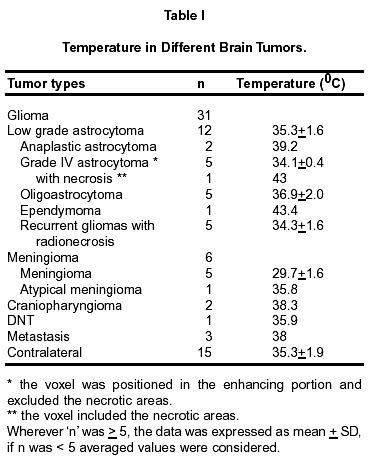
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 436-439 In Vivo Temperature Measurements in Brain Tumors Using Proton MR Spectroscopy R. Jayasundar, V.P. Singh* Departments of NMR and Neurosurgery*,
All India Institute of Medical Sciences,
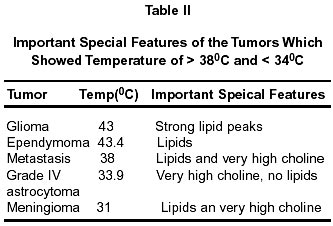
Ansari Nagar, New Delhi - 110 029, India. Accepted for publication : 22nd August, 2001. Code Number: ni02118 Summary The chemical shift difference between the water resonance and the methyl resonance of N-acetylaspartate was used to determine the in vivo temperature in 43 patients with histologically proven brain tumors. Temperatures were also estimated from the contralateral side in 15 of these patients. There was a significant difference (p < 0.05) in temperature between meningiomas and the other tumors viz. low grade astrocytomas, grade IV astrocytomas and oligoastrocytomas. Temperature was also significantly different between the contralateral side and the meningiomas (p < 0.05). Key words : Proton MRS, Brain tumor, Temperature. Introduction Local temperature, in addition to influencing a number of normal biological functions such as protein activity, enzyme-mediated reactions, hemoglobin's affinity for oxygen, etc. is also known to play an important role in diseases.1 For example, even small variations in local brain temperature is known to affect the extent of the injury in brain ischemia.2,3 Knowledge of local temperature can, therefore, provide additional information about the pathophysiology. Magnetic resonance (MR) is an ideal technique to determine the local temperature invivo non-invasively. A number of proton MR parameters such as water relaxation and chemical shift of endogeneous substances have been used in the past for the estimation of temperature in-vivo.4-8 In this study, temperature was estimated in brain tumors, using the chemical shift difference between the water and the methyl resonance of N-acetylaspartate (NAA). Material and Methods Proton MR studies were performed on the Siemens Helicon SP 63/84, 1.5 Tesla MR scanner. The standard circularly polarized head coil was used for both imaging and spectroscopy. Images for localizing volumes of interest (VOI) (< 8 cm3) were acquired in three orientations using the 'turbo-SE' sequence. Water-suppressed proton spectra was acquired from the VOIs using the STEAM pulse sequence with the following spectral parameters: repetition time of 3000 msec, echo time of 135 msec, vector size of 2K points, 4 prescans and 128 acquisitions. Peak areas of NAA, choline (Cho) and creatine/phosphocreatine (Cr) were determined and ratios of the peak areas (NAA/Cho, NAA/Cr, NAA/lipids and Cr/Cho) calculated for these spectra. Spectra, in which NAA was observed were chosen for the temperature estimation. For this study, the transmitter was set at 150 Hz off-resonance from the water signal. The spectra, thus, contained a partially suppressed water signal. The number of acquisitions was 32/64 depending on the strength of the NAA signal. Chemical shift difference between the water resonance (dwater) and the methyl resonance of NAA (dNAA) was used to estimate the temperature (T) using the following equation.8 T = 286.9 - 94 (dwater-NAA )° C 43 patients with intracranial tumors, all of whom underwent surgery, were selected for the study. The tumors were classified on the basis of histological evaluation. The tumors included 31 gliomas (26 primary and 5 recurrent), 6 meningiomas, 2 craniopharyngiomas, 1 dysembryoplastic neuroepithelial tumor (DNT) and 3 metastasis. Of the 31 gliomas studied, there were 12 low grade astrocytomas (grades I and II), 2 anaplastic astrocytomas (grade III), 6 glioblastomas (grade IV), 5 oligoastrocytomas, 1 ependymoma and 5 recurrent low grade astrocytomas with histological evidence of radionecrosis. Temperature was also determined from the contralateral side of the brain in 15 of the patients. A total of 58 spectroscopic studies were carried out. Temperature from the contralateral side of the brain could be estimated only in the patients who were able to lie inside the magnet for a longer period of time. Statistics : Student's paired t-test was used to test the significance of temperature difference between the different tumors and between the tumors and the contralaterals. In all cases, p < 0.05 was considered significant. Relationship between the various metabolite ratios and the temperature was assessed using linear regression analysis. Results The temperature for the different histological types of brain tumors (n=43) and for the contralateral region (n=15) of the patients is presented in Table I. There was no statistically significant difference between the contralateral regions and any of the primary gliomas or the recurrent gliomas with radionecrosis. However, there was a significant difference (p < 0.05) in temperature between the contralateral sides and the meningiomas. Comparing the temperature between different tumors, there was a significant difference (p < 0.05) in temperature between the meningiomas and gliomas (low grade, grade IV, and oligoastrocytomas and the recurrent gliomas). There was, however, no significant difference between the recurrent glial tumors with radionecrosis and the primary gliomas (low grade, grade IV, and oligoastrocytomas). Although, there was no significant difference between the temperature in low grade and grade IV astrocytomas, it should be noted that the mean temperature in the latter is lower than that in the low grade astrocytomas. It is interesting to note that the change in the temperature is not uni-directional as one proceeds from low grade astrocytomas to grades III and IV astrocytomas. Grade III astrocytomas show a higher temperature than the low grade and grade IV astrocytomas. The tumors which had temperature higher than the contralateral side were grade IV astrocytoma (the voxel from which the spectrum was obtained contained necrotic region), ependymoma, craniopharyngioma and the metastatic tumors. The meningiomas had lower values compared to all the other tumors although the high grade astrocytomas also showed a trend towards lower temperature (Table I). The spectral features of the tumors which registered high (> 38°C) and low (< 34°C) temperature values are highlighted in Table II). Of the two types of tumors which registered temperature values < 34°C, the grade IV astrocytoma (n=2) had a very high choline but no lipids and, the meningioma (n=2) had lipids as well as very high choline. All the tumors which showed high temperature (> 38°C) had lipid resonances. The glioma which registered high temperature was a grade IV astrocytoma. The voxel from which the spectrum was obtained contained necrotic areas, which was reflected in the strong lipids seen in the spectrum. It is to be noted that in other grade IV astrocytomas, the voxel was positioned in the enhancing portion and excluded the necrotic areas. The linear regression analysis between the ratios NAA/Cho, NAA/Cr, NAA/lipids and Cr/Cho and the temperature for the different tumors did not show any correlation except in the case of the recurrent gliomas with radionecrosis. In this case, there was good correlation between temperature and NAA/Cr (r=0.99) and NAA/Cho (r=0.9). Discussion Local temperature depends on factors such as the thermoregulatory mechanisms (example blood circulation), and exo-endo-thermic biochemical processes.1 Since these are altered in pathology, it is to be expected that the local temperatures also change in diseased tissues. Estimation of local temperature can, therefore, provide additional information about the disease. Studies on the cerebroprotective potential of hypothermia in pharmacological research, for example, have shown that local temperature has much clinical significance.2,3 Reports on non-invasive in-vivo estimation of local temperatures are very few. Cady et al,8 in their MRS study of piglets and newborn human infants, estimated the temperature in thalamus of 6 newborn human infants to be 38.1+0.4°C. They have shown that the rectal temperature does not reflect the brain temperature and have also demonstrated that while ischemic, the brain temperature fell by upto 2°C relative to the rectal temperature during both normothermia and hypothermia. Tissue, in general, is a poor conductor of heat. Heat transfer in the body depends predominantly on the ability of the organism's circulatory system to remove heat from a given region. Where blood flow to the tumor is significantly less than that in the surrounding normal tissues, thermal energy generated by the tumor metabolism is carried away less rapidly from the tumor than from the adjacent normal tissues. As a result, the tumor temperature rises higher than that of normal tissues. While normal tissue vessels vasodilate in response to increased temperature, thereby increasing the blood flow and further cooling the normal tissues, the tumor vessels are unable to dilate. Hence, the increased temperature is retained in the tumor tissues. On the other hand, when the tumor is hypervascular, the thermal energy produced by the tumor metabolism is carried away efficiently. This results in the tumor having either a normal or less than normal temperature.9 In the present study, difference in temperature has been observed between some of the tumors. Since temperature is regulated mainly through blood circulation, the reason for these differences could simply be the vasculature in the different tumors. If local temperatures can be considered to be closely linked to the vascular supply, then the normal (normal in comparison to the contralaterals) values observed for the low grade astrocytomas are consistent with the absence of any vascular changes for this type of tumors. The low grade astrocytomas are not characterized by any significant vascular changes.10 The anaplastic astrocytomas (grade III) in this study had temperature values higher than the low grade astrocytomas. Of the 12 low grade astrocytomas studied, only one had temperature > 37°C. However, the temperature in both anaplastic astrocytomas was 39.6°C and 38.7°C. Since vascular proliferation is considered limited in anaplastic astrocytomas,10 it is hypothesized that the higher metabolic rate associated with this higher grade tumor in combination with almost normal vasculature could lead to a higher temperature in these tumors. However, more studies are required to substantiate this observation. It is interesting to note that the grade IV astrocytomas had mean temperature lower than that of the low grade astrocytomas. The former not only have a higher metabolic turnover but are also known to be hypervascular.10 These tumors are characterized by rich neovascularity, with vessels that are freely permeable and without the blood brain barrier. Similarly, the meningiomas are also characterized by high vascularity and the temperatures estimated in them are the lowest. Hypervascularity is consistent with lower temperatures observed in these tumors. The temperature estimated in the single ependymoma was high. These tumors are known to have intimal thickening of the tumor vessels leading to gradual occlusion of the vessels.10 This would mean that the heat generated by the altered tumor metabolism cannot be dissipated easily because of the altered and occluded vasculature. This may be the reason for the high temperature. In conclusion, in vivo temperature estimations in brain tumors have been reported for the first time. More such data may prove local temperature to be yet another parameter that may aid the clinicians and help improve the understanding of the tumor physiology. Acknowledgment This work was supported by a grant from Department of Science and Technology, Government of India. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02118t1.jpg] [ni02118t2.jpg] |
| |||||||||

{kind=link}
{kind=link}