 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 440-443 Correlation of Ictal EEG and SPECT Studies in Patients of Intractable Epilepsy with Normal MRI R. Thomas, M. Bhatia, C.S. Bal,* S.B. Gaikwad,** V.P. Singh,*** S. Jain Departments of Neurology, Nuclear Medicine,* Neuroradiology,** Neurosurgery,***
All India Institute of Medical Sciences,
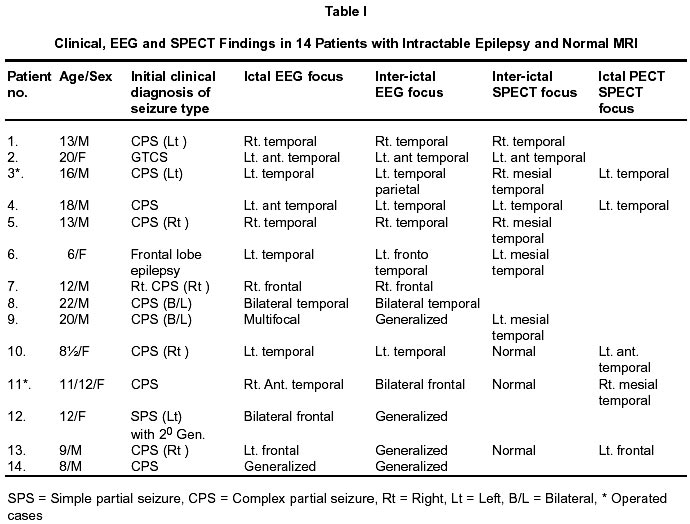
New Delhi - 110 029, India. Accepted for publication : 12th September, 2001. Code Number: ni02119 Summary Identification of the epileptic focus is the most important requirement for a successful surgical outcome in intractable epilepsy. Patients with normal MRI on high-resolution imaging pose a significant challenge in this regard. We tried to identify the epileptic focus using interictal / ictal SPECT and ictal EEG patterns in 14 patients with normal MRI. Rhythmic ictal onset activity helped to identify a single focus in 10 patients (71.43%). Inter ictal SPECT detected a focus corresponding to ictal EEG in 6 out of 10 patients (60%) in whom the test was performed. Ictal SPECT done in 5 patients correctly identified the focus in all patients (100%). Our data indicate that it is possible to obtain localization in patients with normal MRI using a combination of ictal EEG patterns and an ictal SPECT study. Key words : Ictal EEG, SPECT, MRI, Intractable epilepsy. Introduction Surgery for epilepsy is a well-accepted modality for treatment of intractable partial seizures. Identification of the epileptic focus is the most important prerequisite for a successful surgical outcome. This is usually achieved by a combination of detailed clinical evaluation, inter-ictal and ictal EEG studies, structural imaging (MRI) and functional imaging (SPECT or PET). High resolution MRI has emerged as the best diagnostic tool for identification of the epileptogenic lesion. However, in 20-40% of patients with intractable epilepsy, no lesions are detected on MRI.1-3 Invasive EEG studies are extremely useful in these patients in identifying the epileptic focus.4 Recently, however, improvement in the understanding of ictal EEG patterns and perfusion patterns obtained with functional imaging have reduced the need for invasive techniques. Various studies have also found good correlation between EEG patterns, structural and functional imaging data, histopathology and surgical outcome.5-9 In this study, we tried to localize the epileptic focus in patients with normal MRI by means of ictal EEG and correlated them with inter-ictal EEG, and inter-ictal and ictal SPECT patterns. Material and Methods Patients : One hundred fifty seven consecutive patients with intractable epilepsy were evaluated by long-term video EEG from Jan 1998 to Aug 2000 at All India Institute of Medical Sciences, New Delhi. Fourteen patients with normal MRI in the above group were identified and their ictal EEG patterns were studied. The focus obtained was correlated with that of inter-ictal EEG and SPECT studies. MRI : 1.5 Tesla superconducting MRI (Siemens, Magnetom, SP, Germany, Erlanger) was used for the evaluation of epileptogenic lesions. Routine T1 and T2 weighted spin echo sequences were obtained in axial and sagittal plane. T1 weighted inversion recovery and T2 weighted sequences were obtained in coronal plane. Three dimensional volume acquisition images (3 mm slice thickness, 0.1 mm interslice gap) were taken in all the patients. FLAIR sequences were done, whenever it was suggested, after review of the available MRI films by the neuro-radiologist (SBG). MRI was considered normal when no significant atrophy, signal changes or other pathology was observed on visual assessment.11 Inter-ictal EEG : At least 3 (16 channel) inter ictal EEGs of 30 minutes duration, using the 10-20 international system of electrode placement, were done in each patient. Inter ictal record of artifact free awake and sleep EEG of atleast one hour duration available from the long term VEEG, was also analyzed in all patients. The abnormalities identified included spike and sharp wave discharges and area of focal slowing. The area of phase reversal or isoelectric region on bipolar montages12 determined the location of the epileptic focus. Ictal VEEG : All the patients underwent 32-channel video EEG recording. At least 3 habitual seizures were recorded in each patient. Ictal onset and location were defined by the appearance of rhythmic alpha, theta, delta activity or repetitive spikes lasting more than 3 seconds at specific regions. The ictal records were analyzed independently by two experienced electroencephalo-graphers (MB and SJ). SPECT : Nine patients with unilateral foci and one patient with bilateral foci on ictal EEG underwent inter-ictal SPECT study. Five of these patients also had an ictal SPECT study. Inter-ictal studies were performed when patients were seizure free for atleast 24 hours. 15-20 mCi of 99mTc-HMPAO/ECD was injected in each patient using previously described methods.13 Ictal SPECT was studied within 1 minute of the onset of a habitual seizure. An Elscint dual head rotating Gamma camera equipped with fan beam collimator with 3° angular sampling for 360° scanned all the patients within 4 hours of injection. An experienced nuclear physician (CSB) studied transaxial and coronal images. Hypoperfusion or hyperperfusion were recorded, if visually obvious, over at least 3 slices in the region of interest. The foci obtained by ictal EEG were compared with that of inter-ictal EEG, and inter-ictal and ictal SPECT studies. Results Among 157 patients who underwent pre surgical evaluation, 14 were found to have normal MRI. There were 9 male and 5 female patients with a mean age of 12.7 years (range 9 months - 22 years). Twelve patients presented with complex partial seizures. One patient had simple partial seizures and in another the epilepsy was unclassifiable. Review of the clinical symptomatology of the event and ictal patterns helped to identify a single focus in 10 patients of which 8 were temporal and two frontal. Bilateral foci were seen in two patients. Generalized abnormality of no localizing value was found in two patients. Interictal EEG revealed a focus concordant to that of ictal EEG in 7 (50%) patients, bilateral foci in 2 and generalized abnormalities in 5 patients. Of the ten patients who underwent inter-ictal SPECT study, six had an area of hypoperfusion concordant to that of ictal EEG, one had a contralateral focus, and the study was normal in 3 patients. In all patients who underwent the ictal SPECT study, the seizures were observed to persist for atleast one minute after the radiotracer injection was given. Since epileptic focus is seen as region of hyperperfusion during ongoing ictal activity, only hyperperfusion pattern was considered as suggestive of epileptic focus. Ictal SPECT showed a focus concordant to that of ictal EEG in all the five patients in whom the study was done. These five patients, in whom there was good correlation between ictal EEGs and ictal SPECT, were advised surgery. Two patients underwent anterior temporal lobectomy. One patient (Case 3) has remained seizure free during a follow-up period of two years and another patient (Case 11) had significant improvement (> 75% reduction) in seizures during a follow-up period of 1½ years (Table I). Discussion With the standard protocol for high resolution MRI adopted in our study, only 14 of 156 patients (11.15%) had normal MRI studies. It is generally accepted that as many as 40-50% of patients evaluated for frontal lobectomy and 30-40% of those for temporal lobectomy have normal MRI.2 In a study of 128 patients with epilepsy, when high resolution MRI including FLAIR sequences were used, 55 patients (42.9%) were classified as normal.14 The relatively lower incidence of normal MRI in our patients is probably due to the selection bias for video EEG studies, as at our center, patients with a lesion on MRI are given a preference. Identification of the epileptic focus in patients with normal MRI for surgical resection poses a significant challenge. Quantitative MRI using volume measurement of the hippocampus and temporal lobe is a very useful technique for detecting hippocampal atrophy. However, hippocampal sclerosis may be present even when volume studies are normal.15 King et al have also shown, by depth EEG correlative studies, that hippocampal atrophy does not always suggest region of ictal onset.16 Invasive EEG with depth electrodes is generally considered as the gold standard for localization of epileptic foci. It is particularly indicated when MRI shows no abnormalities and functional imaging and non-invasive EEG suggest a focus. Invasive EEG studies have the disadvantage of restricted vision due to limited sampling and may not distinguish between distally propagated seizures and initial discharge of ictal onset zone. Occasionally, complications like hemorrhage and infections may also occur.17 Better understanding of the significance of inter-ictal and ictal EEG patterns and SPECT images have reduced the indications for invasive EEG recording in the localization of epileptic focus. Various authors have observed that repetitive rhythmic activity indicated seizure onset. Risinger et al noted that a 5 Hz or faster rhythm at the temporal region correctly predicted the depth electrode studies in approximately 90% of cases.5 In our patients we used rhythmic alpha, theta, delta or repetitive spike activity lasting more than 3 seconds as indicative of seizure onset at specific regions as also described by 18 et al. Pataraia Using these ictal patterns we were able to detect a single focus in 10 out of 14 patients (71.43%) in our study. Inter-ictal SPECT has only a limited diagnostic value in localization with a sensitivity of 70% and specificity of 36%. Ictal SPECT is much more reliable with sensitivity of 90% and specificity of 77% for temporal lobe epilepsy as compared to pathological findings.19 In the present study, of the ten patients who underwent inter ictal SPECT, 6 patients (60%) had a focus concordant to that of ictal EEG. Ictal SPECT correctly localized the epileptic foci in all the five patients who underwent the procedure. In addition, all 3 cases which had normal on inter ictal SPECT were correctly identified on ictal SPECT. The sensitivity of ictal EEG and ictal SPECT in localization of the epileptic focus have been reported to be 79.4% and 89.7% respectively.20 This study also showed that ictal EEG and ictal SPECT not only have very good correlation but also mutually supplement each other in increasing the diagnostic yield. In our study ictal SPECT had a concordance of 100% and inter-ictal SPECT about 60% when specific regional ictal patterns in EEG were taken as evidence of epileptogenic focus. The surgical outcome of patients with intractable epilepsy and normal MRI has been evaluated in only a few studies. In a study of 19 patients with non lesional temporal lobe epilepsy who underwent surgery only 16% remained seizure free, 42% showed significant improvement and in another 42% no worthwhile improvement was observed.21 The limitation of the present study was that only two patients with non lesional intractable epilepsy underwent surgery. However, both had good surgical outcome. Thus, in patients with intractable epilepsy and a normal MRI, a combination of ictal SPECT and ictal EEG studies may be used for detecting the epileptogenic zone and surgery may be offered as a treatment option to patients of this sub-group. This is of particular relevance in the epilepsy surgery programmes of developing countries where facilities for invasive studies are not commonly available. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02119t1.jpg] |
| |||||||||

{kind=link}