 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 462-466 Oligodendroglioma : Clinical Profile and Treatment Results R. Jacob, R. Jyothirmayi, Y. Dalal,* U. Nambiar,* B. Rajan, M.K. Nair Department of Radiotherapy,
Regional Cancer Center
and
Department of Neurosurgery*,
Sree Chitira Thirunal Institute of Medical Sciences,
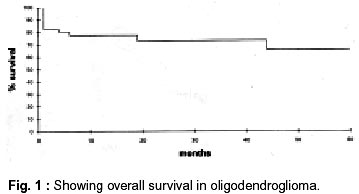
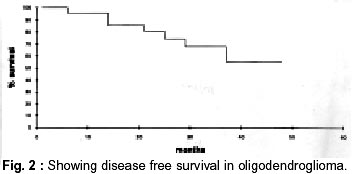
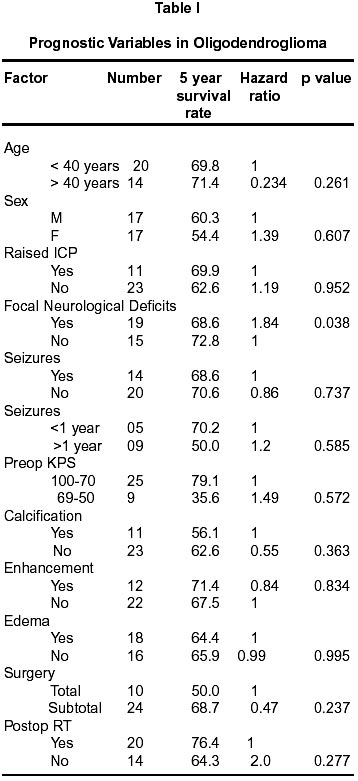
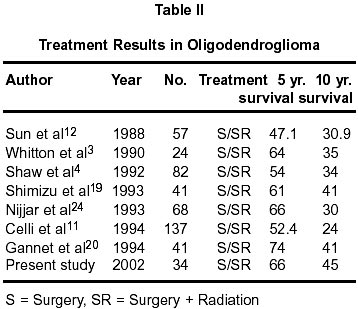
Trivandrum, India. Accepted for publication : 30th January, 2001 Code Number: ni02123 Summary Oligodendrogliomas are rare glial tumors with a long natural history. Radical surgery, postoperative radiotherapy, chemotherapy and observation have been suggested as part of primary management. This series reports the presentation and outcome in 34 patients with histologically verified pure oligodendrogliomas treated between 1983 and 1993. All patients were treated at the time of initial diagnosis with surgery, with or without additional radiotherapy. The overall survival and progression free survival rates at five years were 69.8% and 55% respectively. There was no tumor or treatment related factor influencing survival significantly. Key words : Oligodendroglioma, Radiotherapy, Surgery. Introduction Oligodendrogliomas account for 2-5% of all primary intracranial tumors.1,2 These are slowly progressive tumors with a natural history spanning several years.2 The optimal treatment of oligodendrogliomas is yet to be defined. Radical surgical resection is reported to improve survival, and the role of postoperative radiotherapy is controversial.3,4 The role of chemotherapy is undefined.5 The optimal timing of treatment has not been determined as yet. Observation with delayed intervention has also been suggested as an option.6 This study was aimed at comparing patient profile and treatment results with those reported in the published literature. Material and Methods 34 patients who presented initially at the neurosurgical unit of the Sree Chitra Thirunal Institute of Medical Sciences and Technology, Trivandrum, (SCT) and were diagnosed as pure oligodendrogliomas were included in the study. They underwent detailed neurological evaluation. The preoperative performance status was assessed using the Karnofsky's performance score (KPS).7 Contrast enhanced CT scans were done in all the cases preoperatively. Total excision was the preferred surgical option although partial excision was performed when there was danger of permanent neurological deficits with radical surgery. Kernohan's system8 was used for grading of tumors at the time of initial diagnosis. For the purpose of this study, all tumors were regraded by the same pathologist, based on features of nuclear atypia, mitosis, endothelial proliferation and necrosis. All tumors with necrosis were graded as III. In the presence of one feature, with the exception of necrosis, tumors were graded as I. All other tumors were grouped in grade II. Patients were referred postoperatively to the regional cancer center (RCC) for radiotherapy and combined care. Radiation was delivered using a 4 MV linear accelerator or a cobalt machine. The planning target volume (PTV) included the gross tumor volume (GTV) with a margin of 3 cm. The median tumor dose was 55 Gy (45-55 Gy) in 1.8 Gy fractions (1.6- 2.0 Gy) delivered over 5 to 7 weeks, using a two or three field technique. Chemotherapy was not used in the initial treatment. Patients were followed up jointly at the SCT and RCC at three months interval for the first year and at six months interval thereafter. Diagnosis of disease progression was made on the basis of clinical symptoms and confirmed on CT scans. Patients with recurrent tumors were reoperated, when it was possible to carry out the procedure without producing further neurological deficits. Patients who could not be reoperated were treated with steroids and supportive measures. Chemotherapy was not used for tumor recurrence in our center during the study period. Survival and follow-up were calculated from the date of surgery. The end points for the study were symptomatic local recurrence or death. Survival rates were estimated using the Kaplan Meier product limit method.9 Prognostic factors for survival were analyzed using Cox proportional hazards method.10 Results The mean age at presentation was 28 years (3-58 years), with equal distribution between the sexes (17 each). Headache was the commonest presenting symptom (n=23), followed by seizures (n=14). The mean duration of symptoms was 12 months (1 month - 20 years) for headache and 32.7 months (1 month-20 years) for seizures. Nineteen patients had focal neurological deficits at the time of presentation, which included cranial nerve palsies (13), motor deficits (8), dysphasia and visual deficit (1 each). Twenty three patients (67.6%) had clinical evidence of increased intra-cranial pressure. Twenty five patients (73.5%) had a KPS of 80 or more and 9 had a KPS between 50 and 80. The tumor was supratentorial in all patients, with involvement of frontal lobe in 14, parietal lobe in 3 and temporal lobe in 2 patients. Ten patients (29.4%) had evidence of ventricular involvement. The other sites of tumor included corpus callosum (2) and thalamus, optic chiasm, and pineal region (1 each). The tumors were hypodense on CT imaging in 11 patients, hyperdense in 5 and isodense in 3 patients. The tumors were of mixed density (15) in majority of cases. Contrast enhancement of tumor was present in 22 and tumor calcification in 11 patients. Eighteen patients (53%) had peritumoral edema. Twenty four patients underwent partial excision of the tumor. Complete macroscopic excision of the tumor was done in 10 cases. Two patients underwent surgical re-exploration in the immediate postoperative period for evacuation of hematoma. The mean duration of postoperative hospital stay was 17 days (range 7-90 days). In the initial histology report, 6 tumors were reported as grade II, and one as grade III. Tumor grade was not specified in 27 patients (79%). On review, 26 patients had grade I, 3 patients grade II, and 5 patients grade III tumor. Twenty patients (59%) received postoperative radiotherapy. Fourteen of these had partial excision and 6 had total excision of their tumors. Fourteen patients did not receive radiotherapy either due to poor performance status (8) or patient refusal (6). The remaining the 20 patients completed the planned course of radiotherapy without interruption. Follow-up status was available for 31 of 34 patients. The median follow-up was 68 months (range 1-178 months). Six low-grade and three high-grade tumors recurred locally. The mean time for local recurrence was 26 months (range 8-38 months). All tumors recurred within the field of irradiation. Surgical excision of recurrence was performed in 6 patients who had initial diagnosis of low grade oligodendroglioma. The recurrent tumor was also found to be of low grade. In 3 patients, the extent of recurrence was such that reoperation was not feasible without producing further neurological deficits; hence they were managed conservatively with steroids and other symptomatic measures. The actuarial overall survival was 66% and 45% at 5 and 10 years respectively (Fig. 1). The 5 year progression free survival rate was 54.2% (Fig. 2). The mean time to progression was 32.5 months (range 6 - 111 months). Possible prognostic factors for overall survival were subjected to univariate analysis. Presence of focal neurological deficits at presentation was the only factor influencing survival (HR = 1.84, p = 0.038). None of the other factors, including age, sex, duration of symptoms, frequency of seizures, performance status, contrast enhancement of tumor, tumor calcification, peritumoral edema, extent of surgery, or addition of radiotherapy, influenced survival (Table I). The prognostic significance of the tumor grade could not be assessed, due to the small number of patients with grade III tumors. Discussion There are few published reports of histologically verified pure oligodendrogliomas from this part of the world. The present study was aimed at comparing patient profile and treatment results with published reports. In this study, the patient characteristics and clinical profile are similar to those reported earlier.11-13 In view of the long term morbidity of brain irradiation, it is debatable whether all glial tumors require treatment at the time of diagnosis. Cairncross et al6 recommended careful clinical and radiological follow-up of patients with suspected low grade glial tumors and active management of those with signs of accelerated progression. This is ratified by studies, which show similar results with supra tentorial non-enhancing mass lesions treated either at diagnosis or at the time of progression.14 Low grade oligodendro-gliomas have a natural history similar to low grade astrocytomas, and hence observation and delayed treatment may be recommended for these tumors, also. Despite a contrary report by Celli et al11 demonstrating survival advantage in low grade gliomas treated at the time of diagnosis, delayed treatment is still recommended for low grade oligodendrogliomas, as minor gains in tumor control may be offset by treatment related cognitive impairment and other morbidity.15 This is particularly important in the light of the large number of children presenting with these slow growing tumors. Radical surgical excision of oligodendroglioma has been shown to improve survival rates in several studies.3,4,11 Total and subtotal resection resulted in 5 year survival rates of 74% and 46% respectively.4 Celli et al11 reported better results with subtotal resection as compared to partial removal or biopsy. However, no such relation to the extent of resection was found by Sun et al,12 probably due to the small number of patients treated by surgery alone. The apparent advantage with radical surgery may not be a true one as small tumors without involvement of vital structures are more amenable to radical excision. The exact role of surgery is difficult to establish in the absence of prospective studies. Sheline et al16 and Chin et al2 described the radioresponsiveness of oligodendroglioma in small patient groups. Several workers have reported survival benefit with postoperative radiotherapy.17-19 Gannett et al20 reported a significantly improved survival of 84 months in patients treated with postoperative radiotherapy as compared to 47 months in those treated by surgery alone. Meta analysis by Shimizu et al,19 revealed a 14% improvement in 5 year survival in patients treated with radiotherapy following partial tumor resection. In our series too, patients given postoperative radiotherapy showed a trend towards improved survival. Though some studies have failed to show benefit with radiotherapy, their interpretation is difficult due to widely varying doses and fractionation schedules of radiotherapy used.1,12,21-24 Paleologos et al28 reported 70% response rate with a combination of procarbazine, vincristine and CCNU (PCV) in anaplastic oligodendrogliomas, when used preoperatively. Use of this regime in the preoperative treatment of anaplastic oligodendro-glioma is being investigated in a Medical Research Council UK trial.29 Jeremic et al30 reported 52% 5 year progression free survival in anaplastic oligodendrogliomas using surgery, radiotherapy and adjuvant PCV chemotherapy. Recurrent oligodend-rogliomas treated with the same chemotherapy regime shows upto 63% response rate.31 The 5 and 10 year survival rates of 66% and 45% in our study are comparable to previously published results (Table II). Performance status, intellect and psychomotor function and focal neurological deficits have been identified as significant predictors of survival in several series.1,12,20 All these factors may reflect the extent of disease or involvement of vital areas in the brain. In the present series, presence of focal neurological deficits was an adverse prognostic factor for survival. Calcification of tumor and absence of contrast enhancement have also been reported to be associated with better outcome.18,32 The former may denote the long duration and indolent nature of these tumors. In the present series, tumour calcification, contrast enhancement or peritumoral edema did not emerge as independent predictors of survival. The prognostic significance of histological grading alone may be of limited value in oligodendroglioma. The role of immunohistochemical parameters, like MIB-1, labeling indexes (LI) and staining for glial fibrillary acidic orotein (GFAP), are being studied. It is difficult to evaluate the role of various treatment modalities in oligodendrogliomas due to their relative rarity and long natural history. Most studies are retrospective with small sample sizes and heterogeneous patient population. Multicentric studies may be required to accrue the large sample size needed for assessment of prognostic factors and for elucidating the optimal treatment schedule for these tumors. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02123t1.jpg] [ni02123f2.jpg] [ni02123t2.jpg] [ni02123f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}