 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 467-469 Pitfalls in Diagnosis of Epilepsy of Janz and its Implications S. Jha, V.N. Mathur,* V.N. Mishra Department of Neurology,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
Lucknow - 226 014,
and
Department of Neurology*,
Medwin Hospital,
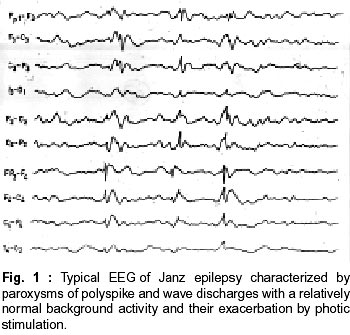
Hyderabad, India. Accepted for publication : 7th November, 2001. Code Number: ni02124 Summary 84 patients of juvenile myoclonic epilepsy (JME) of Janz were studied. Diagnosis was confirmed using clinical and electro-encephalographic (EEG) criterias. 58 (78%) patients of JME were referred as 'refractory or uncontrolled seizures'. Ignoring myoclonic episodes and non-use of activation procedures in EEG were important reasons for diagnostic delay. Sodium valproate (VPA) or clonazepam are the drugs of choice while phenobarbitone (PB), carbamazepine (CZ), and phenytoin (PHT) are ineffective. Clinical spectrum of JME is slightly different in India. Family history of epilepsy or JME is not forthcoming and there is gross delay in the diagnosis. Other differences include age of presentation and mild cognitive impairment. All juvenile patients of generalized epilepsy, not responding to more commonly used CZ, PB and PHT should be strongly suspected for JME by carefully searching for myoclonus. Key words : Myoclonic, Janz, Valproate. Introduction Juvenile myoclonic epilepsy of Janz (JME) is a syndrome seen in puberty and is characterized by bilateral arrhythmic, single or repetitive myoclonic jerks predominantly in arms and shoulders.1 It is diagnostically delayed epilepsy, which is often missed, wrongly labeled or frequently undiagnosed all over the world including India.2,3 Like other epilepsies, it is important to identify JME early, as it has a favorable prognosis. This study was undertaken to share our experience about epilepsy of Janz. Material and Methods The study was conducted on 84 cases suffering from JME, selected after screening 1026 cases of seizure disorder in the age range of 12-24 years. (Mean 16.8+6.1 years). Criteria for Janz epilepsy were: i) typical sequence of absence and myoclonic seizures; followed by generalized tonic clonic seizures (GTCS), ii) diurnal variation of seizures (early morning) and exacerbation by sleep deprivation, hyperventilation, photo flickering and flashing, iii) normal cognition, physical examination and cranial imaging, iv) family history of epilepsy, v) characteristic EEG changes and vi) good response to valproate(VPA) or clonazepam therapy. Four of six criteria were mandatory for inclusion in the study.4 A thorough history (including evaluation of family) and detailed neurological examination was followed by electroencephalogram (EEG) using hyperventilation, sleep deprivation and photic stimulation as activation procedures. Radiological (cranial imaging), and biochemical (hepato-renal and metabolic) evaluation was done to rule out any pathology. These patients were managed on VPA in dose tailored to 20-40 mg/kg bodyweight. Clonazepam (0.01-0.10 mg/kg body weight) was added if they did not become seizure free even with maximum dose of VPA. Patients were followed up till they were free from seizures for a minimum period of 18 months. The duration of study was 5 years. Results Eighty four patients fulfilling the criterias of JME were in the age range of 12-18 years (mean 13.6 ± 3.6 years). No significant sex predilection was seen. Family history of seizures was present in 14 (16%), of which JME was confirmed in only 6 (43%). JME in siblings was observed in only one family. Early morning seizures and precipitation by inadequate sleep (attending late night marriages) was present in 62 (73.8%) patients. Referral diagnosis of 'intractable or uncontrolled epilepsy' was present in 56 (66.6%), while remaining 28 cases (33.3%) reported due to inadequate reduction in seizures. There were 37 (44%) patients on CBZ, 28 (33%) on PHT and 6 (7%) on VPA (inadequate dose) at the time of reporting. There were 4 patients (4.7%) on polytherapy of PB and PHT, 4(4.7%) patients on VPA and PHT and 5 (6%) on CBZ and VPA combination. Mental status evaluation (Folstein's scale) was within normal limits and no clinical evidence of cognitive dysfunction was present in any patient, though there were complaints of decline in scholastic performance in 9 cases. Pathological or radiographical investigations (cranial CT) revealed no focal lesions. EEG was abnormal in all cases. The characteristic EEG changes were in the form of paroxysms of bilaterally symmetrical, frontocentral accentuated polyspike and wave complexes, with relatively normal background activity. Activation procedures like photic stimulation and sleep deprivation exacerbated or precipitated the paroxysm. (Fig. 1). Nearly all (78) patients (93%) responded satisfactorily (>75% reduction in seizures) to VPA, while the rest (8%) responded on adding clonazepam, after failure to respond to maximum dose of VPA (40 mg/kg body weight). All patients were advised to sleep well and avoid working late hours at night. In 6 patients, we attempted to taper the VPA, following complaints of weight gain and alopecia (4 and 2 patients respectively) which had to be restarted following recurrence in myoclonic seizures. Discussion JME is a highly under recognized syndrome, often missed by physicians. Most of these patients are treated for any one component of the syndrome i.e. GTCS or absence, with drugs specific for that particular type of seizure. CBZ, PHT or PB, depending on physician's choice. Unfortunately this results in progressive deterioration and increased seizure frequency. Uncontrolled seizure and trauma may result in decline in cognition, which may explain the complaints of decline in scholastic performance in 9 cases in the series. Family history of epilepsy or JME was not strong in our group of cases. More so, the gross delay in diagnosis, age of presentation and mild cognitive impairment make the clinical spectrum of JME slightly different in India. This is presumably due to : i) poor practice to classify this epilepsy before starting therapy, ii) poor recognition of nonconvulsive seizures like absence and myoclonic jerks, iii) improper evaluation of characteristics of GTCS favouring JME.2,3 The cardinal clinical features for JME are short bilaterally symmetrical and synchronous muscle contractions affecting mainly the shoulder and arm which may be mostly perceived by the patients as an inward electric shock. Because of some peculiar characteristic and favourable prognosis, this epilepsy has attracted lot of attention.5,6 It never produces jerks in individual muscles but only contraction of synergistic group of muscles, while patient is fully conscious. The jerks occur frequently after awakening with toilet objects being flung around; the parents often attributing it to the obstinate attitude of the growing child. Neurological examination is normal. EEG is abnormal but if activation procedures are inadequate, no abnormality may be detected. Sleep deprived EEG must be done in all before labeling an EEG as normal, this being the most important activation procedure. Photosensitivity is a genetically determined bioelectric reaction, which occurs with significantly increased frequency in JME.5,7 The circardian distribution of myoclonic jerks predominantly on awakening in JME is attributed to the disturbance of sleep-wake cycle mediated by mesencephalic and pedunculopontine reticular formation'.1,5 The resultant electrical activity in ascending cholinergic neurons which project to reticulo-thalamic and cortical neurons trigger the cessation of sleep and render the cerebral cortex receptive to sensory impulses on awakening. Moreover, it may be worthwhile to witness the seizure by neurophysicians and obtain an EEG record simultaneously. Misdiagnosis and improper treatment has been reported in various countries and acquaintance with this syndrome is important, since if diagnosed early the prognosis is excellent.6,8 Modifications of sleep, abstinance of alcohol, reduction in intake of nicotine and caffeine have beneficial effects. VPA is the drug of choice.7,9 Many other drugs viz. primidone, PB and Clonazepam have been tried with variable responses of which clonazepam has been reported to produce beneficial effects. It is however one form of epilepsy where discontinuation should be strongly discouraged even if patients are seizure free for long and anti-epileptic medication should be advised to continue life long.9,10 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02124f1.jpg] |
| |||||||||

{kind=link}