 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 470-472 Case Report Naegleria Meningitis : A Rare Survival R. Jain, S. Prabhakar, M. Modi, R. Bhatia, R. Sehgal* Department of Neurology and Parasitology*,
Postgraduate Institute of Medical Education and Research,
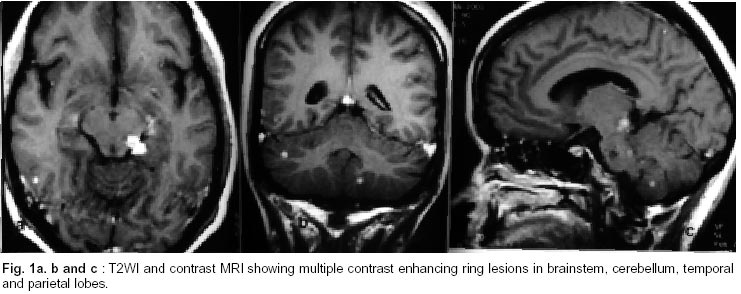
Chandigarh - 160 012, India Accepted for publication : 19th September, 2001. Code Number: ni02125 Summary Acute amebic meningoencephalitis caused by free-living amebae naegleria fowleri is extremely rare and uniformly fatal with only seven survivals reported till date. An interesting case of naegleria meningitis diagnosed by wet mount cytology of cerebrospinal fluid (CSF) and treated with amphoterecin B, rifampicin and ornidazole with complete recovery is presented. In cases of suspected pyogenic meningitis, if CSF staining, antigen detection or culture is negative for bacteria, a wet mount cytology of CSF for naegleria is suggested. Early treatment with amphoterecin B and rifampicin may improve survival. Key words : Naegleria fowleri, Amebic meningoencephalitis Introduction The free living amebae Naegleria fowleri, Acanthemeba species and Bala muthiamandrillaris cause extremely rare and sporadic central nervous system (CNS) infections termed as primary amebic meningoencephalitis (PAM) which were first described in 1965 by Fowler and Carter in Australia.1 Typically, N.fowleri produces an acute amebic meningoencephalitis (AAM) which is clinically indistinguishable from acute bacterial meningitis, where as acanthemeba cause subacute to chronic infection as granulomatous amebic encephalitis (GAE) which may mimic a brain abscess, chronic meningitis or CNS malignancy.2 About 300 cases of PAM have been reported internationally, mostly from US, Australia and Europe. These infections are nearly uniformly fatal with only seven survivors of PAM reported in western literature.3-9 From India, only one survivor of naegleria meningitis has been reported earlier, the present case being the second one. Case Report A 26 year old female presented with history of fever, headache, vomiting and altered sensorium of 10 days duration. Fever was mild to moderate without any associated chills or rigors. Headaches were bifrontal, occipital, nonthrobbing, more in the morning and associated with recurrent episodes of projectile vomiting. Associated neck pain was present. There was no evidence of any cranial nerve involvement, focal deficit, altered sensorium or seizures. Patient neither swam nor had taken any recent bath in pond, pool or lake. All relevant history for tuberculosis was negative. A plain and contrast CT done on 3rd day of onset of illness, revealed multiple contrast enhancing lesions. Following CT, CSF was also examined in a private hospital, which revealed 950 cells/mm3 (P3,L97) with 410 mg/dl protein and 52 mg/dl of sugar and with negative cysticercal serology. Based on CSF, CT and clinical status, she was started on four drug anti-tubercular therapy (ATT), dexamethasone and mannitol. The patient was referred to Postgraduate Institute of Medical Education and Research after a week with no improvement in clinical status. On examination, there was marked neck stiffness and Kernig's sign was positive. Fundus examination revealed a congested disc with reduced venous pulsations. Investigations revealed a TLC of 19,100/mm3 (P88,L10,M1,E1). Repeat CSF analysis revealed 360 cells/mm3 (P20 L80), ADA of 11 units with PCR for tuberculosis, cryptococcal antigen, cysticeral serology, malignant cell cytology, AFB culture, gram stain being all negative. To our surprise, the cytology of wet mount CSF revealed plenty of motile trophozoites of naegleria. The finding was confirmed with a repeat CSF that revealed plenty of actively motile trophozoites consistent with the morphology of naegleria. Amebic culture was negative. CSF PCR for tuberculosis and gram stain were negative on second examination also. Chest Xray, collagen vascular profile, ultrasound abdomen were normal and nasal smear for naegleria was negative. MRI brain (plain and contrast) revealed multiple small enhancing disc lesions with meningeal enhancement (Fig. 1 and 2). Based on the clinical profile and CSF cytology, an aggressive management for acute naegleria meningitis was started. Rifampicin was continued in a dose of 450 mg orally per day. Amphotericin B was started in a dose of 1mg/kg/day with a strict monitoring of renal functions and serum electrolytes. Ornidazole was also added in doses of 500 mg every 8 hour. Steroids were gradually tapered over two weeks. After a week's therapy, there was improvement in clinical signs and symptoms. Repeat CSF after two weeks of treatment was absolutely normal with no evidence of naegleria trophozoites. Treatment was continued for three weeks and later patient was discharged. On follow up, three months later patient was totally asymptomatic. Discussion Primary amebic meningoencephalitis is divided into acute amebic meningoencephalitis (AAM) and granulomatous amebic encephalitis (GAE). AAM is principally caused by N.fowleri in a patient with excellent health with prior intimate contact with fresh water, especially in summer months. The portal of entry is via the olfactory mucosa and neuroepithelium. Incubation period is 3-8 days with acute and rapidly fatal course. Patient usually dies within 7-10 days of onset of symptoms. Clinical picture resembles acute bacterial meningitis.2,10,11 Diagnostic test involves CSF study with direct visualization of naegleria under light microscope which are actively motile and can be stained with Heidenhain's iron hematoxylin and Wheatley's trichrome stain.2. There is pleocytosis with neutrophilic dominance and a high protein with low sugar. Indirect hemagglutination, ELISA, indirect /direct immunofluorescence are other methods used for diagnosis. However, serology is not useful in diagnosis during the acute stage, as antibodies to naegleria species have also been detected in normal person.12,13 MRI is usually suggestive of cerebral edema with meningeal enhancement.14 The drug of choice is amphotericin-B (intra thecal and intra venous). Rifampicin, tetracyclin may be added for better results. Although amoebicidal drugs as metronidazole and ornidazole have no activity against free living ameba, we still used it in view of the atypical presentation of the index case and their good efficacy against cerebral amebiasis. All the survivors reported till date were treated with amphotericin B. In contrast, GAE is caused principally by acanthameba species especially in immunosuppressive hosts. The course is subacute to chronic but is terminally fatal. Usually the trophozoites are not seen in CSF smear and cytology usually reveals a lymphocytic pleocytosis. MRI reveals multifocal contrast enhancing lesions with predilection for diencephalon, thalamus, brain stem and posterior fossa structures.2,14,15 Naegleria infection has also been reported from other sources such as tap water and air.16,17 Sub- clinical infection due to naegleria may occur in a healthy individual when these amebae colonise the nose and throat.18 The index case presumably acquired infection from air and had a subacute course similar to the other survival of naegleria meningitis reported from India.10 MRI and CT pictures in this case were more suggestive of GAE instead of AAM. Although CSF had shown plenty of actively motile trophozoites suggestive of naegleria infection, but the presence of lymphocytic pleocytosis is unusual. In view of the fact that the present case had features of both naegleria meningitis as well as a subacute to chronic granulomatous disease caused by acanthameba, two possibilities emerge. Either the patient was having a mixed infection, which seems less likely or a lesser virulent strain of naegleria was responsible for the same. In conclusion, although PAM is rare and has poor prognosis, it should be considered in any patient of pyogenic meningitis without evidence of bacteria by staining, antigen detection and culture. CSF cytology of wet mount becomes mandatory in such cases as early treatment with amphotericin may improve survival. Reference
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02125f1.jpg] |
| |||||||||

{kind=link}