 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 487-489 Case Report Bereitschaftspotential in Tic Disorders : A Preliminary Observation H.S. Duggal, S.Haque Nizamie Department of Psychiatry,
Central Institute of Psychiatry,
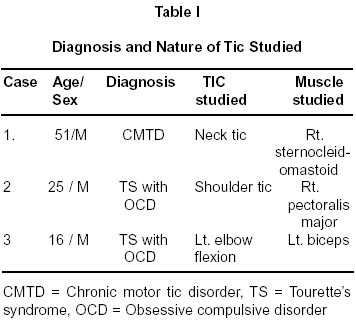
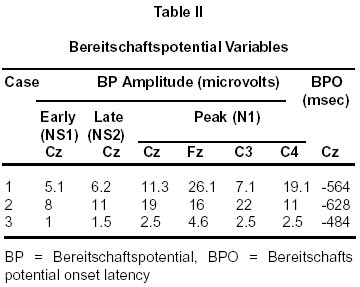
Kanke, Ranchi - 834 006, India. Accepted for publication : 24th January, 2001 Code Number: ni02130 Summary Sensory phenomena in tic disorders such as Tourette's syndrome are known but are substantiated by only a handful of studies. In this preliminary report, we studied premonitory urge, a type of sensory phenomenon in three patients of tic disorders. Bereitschaftspotential, a movement-related cognitive potential indicative of motor preparation, was assessed in these patients. As bereitschaftspotential was observed in all our cases prior to occurrence of tics, it is speculated that tics are not entirely involuntary but are quasi-volitional in nature. Bereitschaftspotential may thus represent a neurophysiological marker of premonitory urge in tic disorders. Implications of exploring the voluntary nature of tics are discussed. Key words : Bereitschaftspotential, Tic disorder, Premonitory urge. Introduction Tourette's syndrome (TS) has traditionally been described as a hyperkinetic movement disorder characterized by involuntary motor and phonic tics. ICD-10 defines tic as an involuntary, rapid, recurrent, non-rhythmic motor movement or vocal production, which is of sudden onset and serves no apparent purpose.1 It is an accepted notion in classical literature that tics are involuntary, however, there have been reports which have challenged this dogmatic view. The volitional component of tics was first highlighted by a patient of TS himself who explicitly described sensory experiences preceding or occuring during the tics.2 Subsequently, other investigators have examined the sensory phenomena associated with tics.3-6 Some investigators have classified sensory phenomena as bodily sensations and mental sensations.6 A premonitory urge is a drive to perform the repetitive behaviour. It is a force or impulse without any obsession, fear, worry or bodily sensations. In this study, we chose to study premonitory urge in patients with tic disorders as it is quite common in these patients with one study reporting a prevalence of 82%.3 Bereitschaftspotential (BP) is a movementrelated potential, a negativity occurring in the baseline EEG of a subject when he carries out a self-paced movement. This potential denotes the cortical preparation in advance of the actual voluntary movement. BP is a psychophysiological marker of movement planning and decision-making,7 and is divided into two main components-the early and late BP.8 In patients who report a premonitory urge preceding the tics, there is awareness of the oncoming movement. The aim of this study to explore whether BP can serve as a neurophysiological correlate of this premonitory urge. Material and Methods Three patients who met the ICD-10 criteria for either Tourrete's syndrome or chronic motor tic disorder were studied. All the subjects had premonitory urge preceding the tics, which was assessed using a questionnaire.3 After an informed consent, the patients underwent recording for BP. The protocol followed was similar to that of Shibasaki.9 The EMG was recorded from a pair of silver-silver chloride electrodes, placed over the skin overlying the muscle maximally involved in the tic movement. The EMG signals from the muscle triggered the on-line averaging of EEG potentials. The EEG was recorded from four electrode positions of the 10/20 system (Fz, Cz, C3 and C4). The BP curves were obtained by averaging at least 200 artifact free sweeps. The following parameters were defined10 : (a) peak BP negativity (N1), (b) early component of BP (NS1) which was marked visually at the point of transition of early into late BP, (c) lateralized component of BP (NS2) which was calculated by subtracting the NS1 from the peak negativity (N1). BP onset latency (BPO) was defined as the onset of negative potential rise and identified by eye as the point at which the average EEG deviated from the mean baseline activity. Results The clinical and BP variables of the three patients are shown in tables I and II. While the two patients with TS had comorbid obsessive-compulsive disorder (OCD) (according to ICD-10), the patient with chronic motor tic disorder had obsessive-compulsive symptoms not amounting to disorder. BP was recorded in all the patients preceding the tic movement with clear demarcation into early and late components. The BP onset latency (BPO) was, however, shortened in all the subjects (normal = -1000 to -1600 msec). Discussion This preliminary endeavour demonstrates that tics are preceded by cortical activation, which indicates that they have a volitional component. Since all our patients had a premonitory urge, the BP may represent a neurophysiological marker of this phenomenon. Two previous studies have assessed BP in tic disorders. In one study,11 no pre-motor negativity was obtained in six patients with TS. In the other study,12 BP was recorded in two out of five patients of tic disorders. Interestingly, in the latter study, of the two patients showing presence of BP preceding the tics, one had premonitory urge. Our results are more in line with this study. The discrepancy between our findings and those of the first study11 could be due to difference in patient characteristics, as all our cases had obsessive-compulsive behaviour and premonitory urge is more prevalent in patients of tic disorders with OCD.6 Moreover, this study did not mention whether or not patients experienced a premonitory urge, which was the substrate of interest in our study. Voluntary movements have been classified as either intentional (planned or self-induced) or responsive (generated in response to an external stimulus).13 BP is absent in responsive movements while it is present in intentional movements.14 Taken together with our observation, this translates into tics resembling more to intentional voluntary movements than to responsive movements, a view differing from the aforementioned two studies.11,12 However, there is no justification to label tics to be purely voluntary. This derives from the fact that BP onset latency in all our subjects was considerably shortened. Thus, tics at the most represent a quasi-volitional movement. Study of volitional aspects of tics by way of documenting objective evidence of presence of premonitory urge is helpful in the following ways: i) In one study more than half of the subjects with TS reported that the premonitory urge was more bothersome than tics per se.3 ii) Presence of premonitory urge can enhance the patient's ability to suppress tics.3 iii) The premonitory urge is amenable to pharmacological treatment as neuroleptics decreased the frequency and intensity of the premonitory urge.4 Besides the clinical implications of studying premonitory urge in tics as mentioned above, this study provides further insights into the neuroanotomical correlates of this phenomenon. Generators of BP consist of parts of motor cortex, including supplementary motor area and primary motor cortex with inputs from basal ganglia.15 When viewed in the light of involvement of cortico-striatothalamo- cortical circuits in TS and premonitory urge,3 it appears that both BP and TS may share some commonality in neuroanatomical origin. Thus, any abnormality of basal ganglia manifesting as tics may be reflected in abnormal BP as suggested by decreased BP onset latency in our subjects. Therefore, it can be speculated that a shortened BP onset latency may represent a neurophysiological marker of tics in patients with a premonitory urge. These findings need replication in a larger systematic study. A limitation of this study is that we did not compare our findings with BP assessed in voluntary movements simulating the tics as done by previous studies.11,12 Future studies assessing tics and obsessive compulsive symptoms on rating scales and measuring BP across various populations such as chronic tic disorders with or without OCD and in tic disorders with and without premonitory urge would be more fruitful. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02130t1.jpg] [ni02130t2.jpg] |
| |||||||||

{kind=link}
{kind=link}