 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 490-493 Case Report Hemorrhagic Necrosis of Pituitary Adenomas A.G. Chacko, G. Chacko, M.S. Seshadri,* M.J. Chandy Department of Neurological Sciences and Endocrinology*,
Christian Medical College and Hospital,
Vellore - 632 004, India. Accepted for publication : 31st January, 2001. Code Number: ni02131 Summary A clinicopathological study of 41 cases of pituitary apoplexy in a series of 324 surgically treated pituitary adenomas is presented. In 23 patients, the predominant operative finding was hemorrhage with or without necrosis. However, there were 15 (37.7%) cases where pale, necrotic tissue with no evidence of hemorrhage was found at surgery. Pale, necrotic material was particularly found when there was a long interval between the acute clinical event and surgery. It is concluded that the pale, necrotic debris represents one stage in the resorption process of blood after hemorrhagic necrosis of pituitary adenomas. This entity needs to be kept in mind especially since the material closely resemble the pultaceous material seen in craniopharyngiomas and epidermoid cysts Key words : Pituitary adenomas, Apoplexy, Infarction, Hemorrhage. Introduction It is well known that apart from progressive visual and endocrine dysfunction, pituitary adenomas may present as an acute, fulminant neurologic illness commonly called 'pituitary apoplexy'. Although the typical gross and microscopic finding anticipated at surgery was of hemorrhagic necrosis or hemorrhage in a pre-existing pituitary adenoma, we encountered a group of patients in whom pale, necrotic material was seen without evidence of hemorrhage. This group manifested with a clinicoradiological syndrome indistinguishable from that due to hemorrhage. We present the clinicoradiological, surgical and histopathological correlates of this entity, to highlight its occurrence and to determine its pathogenesis. Material and Methods The clinical material consisted of 324 consecutive pituitary adenomas operated through the transsphenoidal route at the Christian Medical College Hospital at Vellore between 1983 and 1995. The operation records were reviewed to identify pituitary adenomas that had altered blood, necrotic material or cystic collections at surgery. Forty-one (12.3%) patients with these intraoperative findings were found. The positive history of an acute episode and the duration between onset of symptoms and surgery were determined from the in-patient records. The patients were divided into four groups, according to the operative findings. When the tumor tissue was pale, pultaceous and necrotic, similar to the findings in epidermoid cysts, the patients were placed in group I (pale, necrotic tissue) ; Those showing both hemorrhage and necrotic material were grouped in group II. Those who had altered blood alone were included in group III, while group IV included patients with cyst with xanthochromic fluid. The biopsy material from these 41 cases was reviewed in detail. Immunostaining using the peroxidaseantiperoxidase technique of Sternberger et al1 was carried out only on those tumors that had viable tumor tissue. The adenomas were graded from the computed tomographic (CT) and magnetic resonance scans according to the system proposed by Hardy and modified by Wilson.2 Results There were 28 male and 13 female patients with age ranging from 18 to 65 years (mean 40.44 years). Clinically, there were 4 growth hormone secreting tumors, 3 prolactinomas and 34 non-functional tumors. CT revealed grade A tumor in 4, grade B in 13, grade C in 16, grade D in 2 and grade E in 6 tumors. Clinical features of the acute event : Twelve patients gave no history of an acute event before seeking medical attention and were asymptomatic for the apoplexy. In the symptomatic patients, the acute presentation of headache, vomiting, loss of consciousness, visual deterioration and ocular motor palsies was similar in all the four groups. In group I, all except one patient gave a history of an acute episode. Nine (60%) of the 15 patients in this group had hypopituitarism including one whose acromegalic features regressed following the 'apoplexy' that occurred three months before admission. The incidence of hypopituitarism in the other groups was 65.3%, with 17 of 26 patients requiring replacement drugs. All 3 patients in group IV (cysts with xanthochromic fluid) were asymptomatic for the apoplexy. Interval between acute episode and surgery : The
interval between the acute event and surgery was
compared in all the groups after excluding the 12
asymptomatic patients. Of the 15 patients with
hemorrhage or hemorrhagic necrosis (groups II and
III), 14 had symptoms for less than 8 weeks prior to
surgery. However, the duration between onset of
symptoms and surgery was more than 8 weeks in 13
of the 14 symptomatic patients in group I. There was,
therefore, a 13 times greater chance of finding pale
necrotic material at surgery when the duration of
symptoms exceeded 8 weeks (Greenland, Robbins
95% confidence limits for relative risk
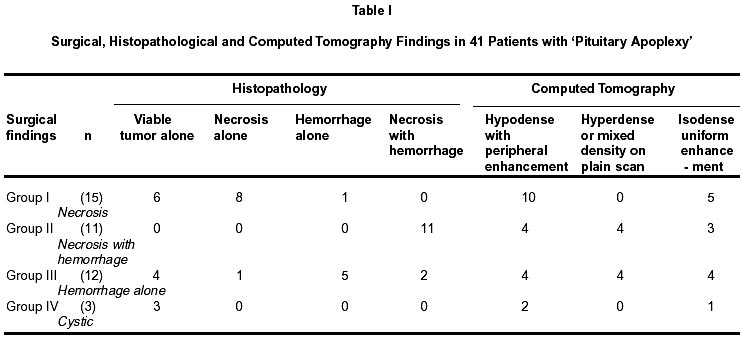
1.99 Surgical and Histopathological findings (Table
I) : Of
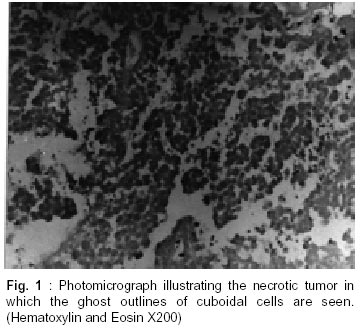
the 15 patients in Group I, 8 were confirmed to have
only necrosis as evidenced by the presence of
acellular eosinophilic material in which the ghost
outlines of cuboidal tumor cells could be seen in some
cases (Fig. 1). There was no microscopic evidence of
recent or old hemorrhage nor was there viable tumor
present. Of the remaining 7 cases, one showed
microscopic evidence of old hemorrhage while in 6
patients only the capsule with scanty viable tumor
tissue was seen. Necrotic material was not present in
these 7 cases, although seen peroperatively and was
probably aspirated at surgery and not submitted for
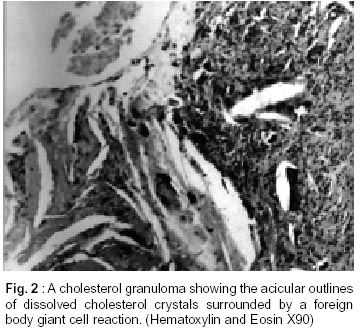
histopathology. All 11 cases in Group II showed old hemorrhage with
cholesterol granulomas and hemosiderin pigment in
addition to necrotic material similar to that seen in
Group I (Fig. 2). In Group III, the finding of recent
hemorrhage was confirmed in all except five.
Immunohistochemistry was possible in only 13 of 41
specimens (32.5%), one tumor was positive for
growth hormone, 3 for prolactin, 1 for
adrenocorticotrophin hormone and 10 were negative
for these hormones.
Radiological appearance : Table I shows the
computed tomogram (CT) findings in the 41 patients
with pituitary apoplexy. The cases that had pale
necrotic material at surgery (Group I) could not be
predicted based on the CT appearance. However,
when the CT scan showed hyperdense or mixed
density lesions on the plain scans, the most probable
intraoperative findings were hemorrhagic necrosis or
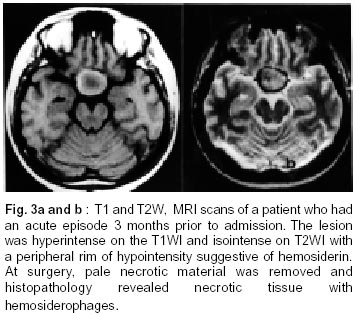
hemorrhage. In group I, 4 patients had MRI scans. The
lesions were isointense on the T1 and hyperintense on
the T2WI in 3 cases, while one lesion was
hyperintense on the T1 and isointense on the T2W
scans, with a hypointense ring at the periphery
suggestive of hemosiderin (Fig. 3a and b).
Discussion Pituitary apoplexy is an acute clinical syndrome
caused by hemorrhage and necrosis in the pituitary
gland. The term has also been applied to similar
pathological changes occurring in pituitary adenomas.
In our series of 324 pituitary adenomas, 41 patients
(12.3%) had surgical or histopathological evidence of
hemorrhage with or without necrosis. Of these, 29 had
symptoms of an acute event. This study focused on 15
patients (37.7%) in whom pale, necrotic tissue with no
hemorrhage was found at surgery. Symptomatic
hemorrhagic infarction in pituitary adenomas has
been reported to occur in 6 to 10% of large series.3
While most of the literature on pituitary apoplexy
describes hemorrhage into or hemorrhagic necrosis of
pituitary adenomas,3-11 non-hemorrhagic
necrosis has
not been considered in detail.3
Rovit et al12 hypothesized
that acute pituitary
apoplexy was the result of the sudden ischemia,
necrosis and hemorrhage in an expanding pituitary
adenoma rather than primary bleeding into a vascular
adenoma. The impaction of the enlarging tumor in the
region of the diaphragmatic notch thus comprises its
afferent blood supply. However, Cardoso et al13 do
not
agree with this theory since angiographic studies show
that pituitary adenomas derive their blood supply not
from the superior hypophyseal artery, but from the
inferior hypophyseal artery which does not get
compressed against the diaphragm. Moreover, there is
electron microscopic evidence of abnormal
fenestration of tumor vessels with fragmented basal
membranes that may predispose to hemorrhage.14 In
our series, since all tumors were macroadenomas with
suprasellar extension, another possible explanation for
the apoplectic event is the tumor outgrowing its blood
supply resulting in sudden expansion of the sellar
mass with the hemorrhage or necrosis. The
histopathological picture, in some of our cases, of
ghost outlines of tumor cells, implying ischemic
necrosis (infarction) lends credence to this
mechanism. Speculating on the natural history of pituitary
apoplexy, Mohr and Hardy15 proposed that cystic
adenomas and the empty sella syndrome may be the
result of hemolysis and resorption of blood
degradation products. They suggest that these entities
represent late stages in the pathological course. We
found that the acute symptoms in group I (pale,
necrotic tissue) were no different from those seen with
hemorrhagic infarction of pituitary adenomas.
However, when the interval between the apoplectic
event and surgery was long (> 8 weeks), pale
infarction was the most likely intraoperative finding.
Whereas, when this interval was less than 8 weeks,
evidence of hemorrhage was seen. This suggests that
pale necrotic debris may represent one of the stages in
the resorption process following hemorrhage or
hemorrhagic necrosis. Indeed, in one of our cases,
MRI showed a hypointense ring on the periphery of
the tumor suggestive of hemosiderin. In this patient,
pale necrotic tissue was found at surgery and at
histopathology a predominantly necrotic tumor was
seen with hemosiderin pigment and cholesterol
granules. In conclusion, the surgeon must be aware of the
natural history of hemorrhagic necrosis of pituitary
adenomas as pale necrotic tissue found at surgery may
be mistaken for the white, pultaceous material seen in
epidermoid cysts and craniopharyngiomas. This issue
is, however, resolved on biopsy as the white, cheesy
material seen intraoperatively in the case of
epidermoid cysts and craniopharyngiomas
corresponds to keratin. References Copyright 2002 - Neurology India.
Also available online at http://www.neurologyindia.com |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}