 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
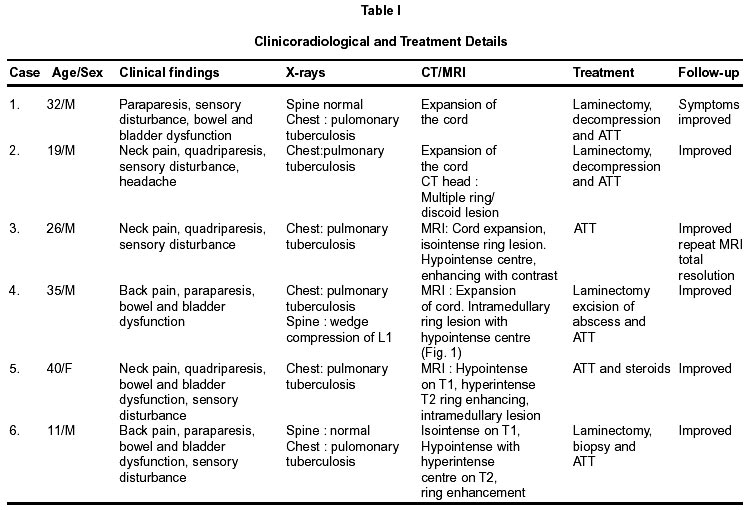
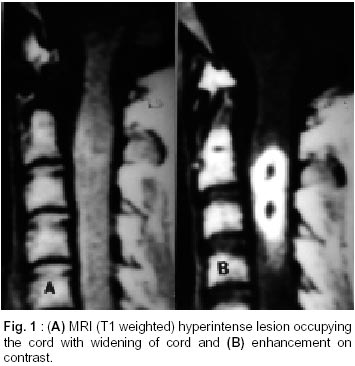
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 494-496 Case Report Spinal Intramedullary Tuberculoma and Abscess : A Rare Cause of Paraparesis B. Indira Devi, S. Chandra, S. Mongia, B.A. Chandramouli, K.V.R. Sastry, S.K. Shankar* Department of Neurosurgery and Neuropathology*,
National Institute of Mental Health and Neurosciences,
Bangalore - 560 029, India. Accepted for publication : 19th July, 2001. Code Number: ni02132 Summary Five cases of spinal intramedullary tuberculomas (IMT) and one case of spinal intramedullary tuberculous abscess (ITA) are presented. Gd enhanced MRI revealed ring enhancing lesion with central hypodensity, suggesting granulomatous pathology. Surgical excision of the intramedullary lesions was carried out in four cases, while two patients received presumptive anti-tuberculous chemotherapy only. Repeat MRI after completion of anti-tuberculous therapy showed total resolution of the lesion. In other cases following surgical excision, the patients improved significantly. The management of these rare lesions is discussed and the literature reviewed. Key words : Intramedullary, Spinal, Tuberculoma, Tuberculous abscess. Introduction Intradural spinal tuberculomas comprise about 2-5% of spinal tuberculosis,1 while intramedullary spinal tuberculomas (IMT) are still rare,2 the incidence quoted being 2 in 100,000 cases of all tuberculosis.3 Spinal intramedullarly tuberculous abscess (ITA) is still rare.4 The clinical presentation and management of five cases of intramedullary spinal tuberculomas and one case of intramedullary tuberculous abscess are presented. Case Report A retrospective analysis of hospital records of neurosurgical services at National Institute of Mental Health and Neurosciences, India, over past 15 years (1985-2000) revealed five cases of intramedullary tuberculomas and one case of intramedullary tuberculous abscess. All the cases were HIV seronegative. Details of the cases are given in Table I and Fig. 1. A total number of 1030 cases of spinal tuberculosis and 8300 cases of intracranial tuberculosis were treated in the neurological services during the study period. This incidence of spinal intramedullary tuberculoma was 1 in 175 cases of spinal tuberculosis and 1 in 1600 cases of nervous system tuberculosis. Histopathology : Histopathological examination of the excised material in all the operated cases showed tuberculomas having multiple epitheloid cell granulomas with Langerhan's and foreign body type of giant cells. Large areas of caseous necrosis were seen. Along the margin of the lesion, ill-formed granulomas admixed with mononuclear infiltrate and gliosis was seen. Variable number of acid-fast bacilli were detected in the lesions. Histological section from one of the cases showed wall of a chronic abscess densely infiltrated by lymphocytes, plasma cells and histiocytes. No distinct granulomas were seen. The cavity contained necrotic material and occasional acid fast bacilli close to the wall, confirming it to be a tuberculous abscess. Discussion Intramedullary spinal tuberculomas (IMT) are rare,5 even in geographical areas where tuberculosis is endemic. The first report of lMT was byAlbercrombie in 1828.1 A total of 148 cases were reported in two reviews. Two cases of IMT were reported in patients with AIDS.6 All the cases, in the present study, were HIV seronegative. Most of the patients with IMT were in younger age group, the average in one series being 23 years.5 This was true in our cases too. Intramedullary tuberculosis is almost always secondary to pulmonary tuberculosis but some cases may present only with isolated extrapulmonary forms.1,5 In the present study, all the patients had evidence of pulmonary tuberculosis detected at the time of initial presentation. One patient, in addition had multiple intracranial tuberculomas detected by cranial CT scan. Concurrent occurrence of intracranial tuberculomas along with intramedullary spinal tuberculoma, though possible, is rare.7 MRI especially with Gd-DTPA has significantly helped in the diagnosis of IMT.8 A common finding on MRI has been spinal cord swelling which regresses after specific antituberculous treatment.2,9 MRI in all the above cases was performed without Gd-DTPA and it was difficult to differentiate IMT from myelitis. Tuberculoma is an evolving granuloma in the nervous tissue, hence it becomes necessary to have Gd-DTPA MRI, with a good follow up, to delineate varying characteristics in evolution. In the initial phase of tuberculoma formation, one finds chronic granulomatous inflammation with formation of giant cells, which homogenously enhances with contrast due to break down of blood-brain barrier. Collagen subsequently gets deposited along the capsule of the tuberculoma and the contents of the lesion get transformed into caseous material. The homogenously enhanced initial lesion becomes a ring-enhanced lesion at this stage. On treatment with chemotherapy the lesion regresses in size and disappears, to be replaced by an area of gliosis, which probably is seen as an area of hypointensity on MRI. Follow-up MRI features, after presumptive chemotherapy, have been reported in only four cases.7,11 In two of the five cases reported here, (case nos. 3 and 4), plain MRI showed cord swelling with some signal changes within the cord suggesting an intra medullary mass lesion or myelitis. The lesions were clearly delineated on Gd- DTPA-enhancement, showing ring lesions with central hypointensity. Follow-up MRI done after one year showed total resolution except for a small speck of hypointensity. Intramedullary spinal tuberculous abscesses is quite rare. A total of only 77 cases of intramedullary abscesses have been reported, since the original case documented by Har.4 Various organisms have been isolated but mycobacterium tuberculosis has been demonstrated in only four cases.4,12 Intramedullary tuberculous abscess may be diagnosed by presence of acid-fast bacilli within the tissue or by positive cultures. MRI in these cases showed signal changes within the cord with expansion of the cord. Gd-DTPA study clearly demonstrated the ring lesion typical of an abscess.13 It may be however difficult to differentiate an intramedullary tuberculous abscess from intramedullary tuberculoma. The MRI of ITA in our case was also similar to that of intramedullary tuberculoma. Presently specific antituberculous chemotherapy is the primary modality of management,9 although the previous authors advised surgery for all symptomatic cases.1,2 Though the response to antituberculous chemotherapy is usually good, paradoxical increase in size of the lesion with treatment may occur necessitating surgical intervention.14 Surgery in the treatment of spinal intramedullary tuberculomas may be indicated for a) large lesions with rapid deterioration of the neurological status, b) non-specific neuroimaging features, c) paradoxical increase in the size of the lesion following antituberculous therapy. Conclusion In endemic regions, intramedullarly spinal lesion in patients with evidence of tuberculosis else-where, could be of tuberculous etiology. Gd-DTPA enhanced MRI can significantly increase the diagnostic accuracy of IMT in conjunction with radiological and serological evidence of tuberculosis. Follow-up MRI becomes essential not only to assess the efficacy of treatment but also to detect paradoxical increase of size if present. These lesions usually have a good response to medical treatment, and if diagnosed early would avoid unnecessary surgical intervention. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02132f1.jpg] [ni02132t1.jpg] |
| |||||||||

{kind=link}
{kind=link}