 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 497-499 Case Report Tuberculoma en Plaque : A Case Report S. Dubey, B. Indira Devi, V.K. Jawalkar, D.I. Bhat Department of Neurosurgery,
National Institute of Mental Health and Neurosciences,
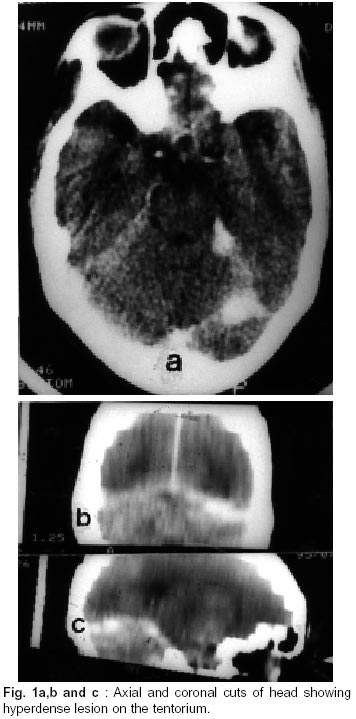
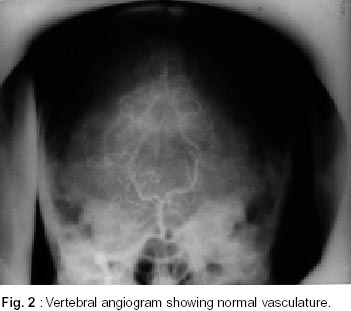
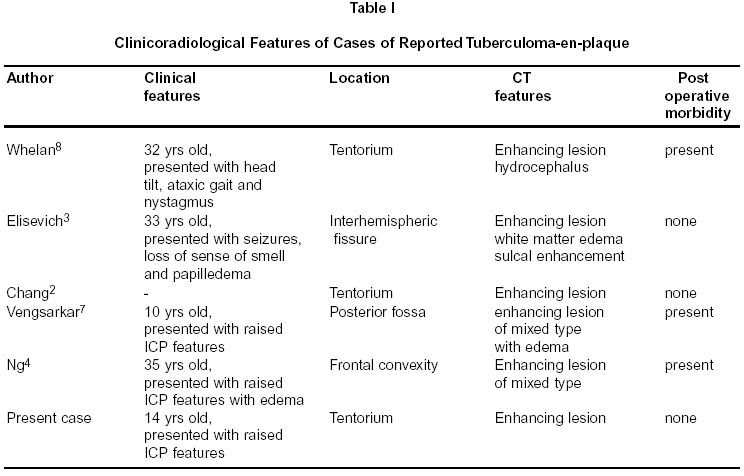
Bangalore - 560 029 India. Accepted for publication : 7th September, 2000. Code Number: ni02133 Summary A 14 year old girl presented with a 6-month history of headaches and visual blurring. CT showed a right tentorial enhancing lesion. Angiogram showed no enhancement. Histopathological examination of the excised material was consistent with tuberculoma. The presentation of such unusual intracranial tuberculoma is reported and the literature reviewed on the subject. Key words : Leptomeningeal tuberculoma, Meningioma, Tuberculoma en plaque. Introduction Intracranial tuberculoma usually results from the hematogenous seeding of the tubercle bacilli to the leptomeninges and brain parenchyma, resulting in formation of tubercles which enlarge and coalesce and are walled by a fibrous capsule. The leptomeningeal tubercles may rupture into the subarachnoid space forming a Rich's foci, resulting in meningitis or may remain confined to the meninges forming a hard fibrous mass attached to the dura i.e., tuberculoma-enplaque. The brain tuberculomas become walled from the surrounding parenchyma by a thick fibrous capsule, and may reach considerable size before symptoms ensue and rarely they may also burst into the subarachnoid space. Clinically, they may be categorized into two groups; those having signs of increased intracranial pressure with or without localizing neurological signs, and those with progressive neurological disability in the absence of elevated intracranial pressure.1-3 Case Report A 14 year old girl presented with headache and visual blurring of 6 months duration. Headache was present throughout the day and sometimes disturbed the sleep. Visual blurring was for both near and far objects, without any history of double vision or field defects. There was no history of fever or neck stiffness. On examination, she was afebrile and her neck was supple. Fundus showed evidence of bilateral papilledema. There were no other neurological deficits. Cranial CT showed right tentorial enhancing lesion without any evidence of hydrocephalus or draining veins (Fig. 1a,b and c). Tentorial based AVM was suspected radiologically and patient underwent four-vessel angiogram, which was negative (Fig. 2). Lumbar CSF examination was non informative. She underwent right suboccipital craniectomy and the biopsy of the tentorial lesion. On surgery the cerebellum was found to be normal, which was retracted to expose the mass attached to dura. Subtotal excision of yellowish relatively avascular lesion was done. Histology was suggestive of tuberculoma. Patient was started on isoniazid, rifampicin and pyrazinamide and at follow up was asymptomatic. Discussion Intracranial tuberculomas have been described in both infratentorial and supratentorial compartments. Tuberculoma en plaque is an unusual form, described first in 1927 by Pardee and Knox as plaque like meningitic process without exudation, usually in the frontal and the parietal region. The gross lesion is essentially localized and very solid without calcified or caseous areas.3,4 In pre CT era it has been described by Sinh et al5 and Thrush et al.6 With the advent of CT, it has been reported regularly in the literature (Table 1). Clinically it is seen in adults and is characterized by a lengthy course. The clinical features depend on the location and include headache, blurring of vision, vomiting, focal seizures, weakness of limbs and neck tilt. The optic fundi are usually normal. Fever is usually, though not neccessarily present and has often constituted an important clue to the diagnosis. Radiologically, on X-rays there is very low incidence of intracranial calcifications but one instance of hyperostosis and sclerosis of the surrounding bone has been described.3 Sometimes, wide dural attachments have been demonstrated with an enlargement of feeding meningeal arteries leading to the lesions.6 Contrast enhanced CT shows characterstic patterns of tuberculomatous lesions.3,4,7,8 Tuberculomas usually falls into three types: i) solid enhancing lesions (tuberculoma en plaque fall into this group though they may have lucent centre or small specks of calcification), ii) ring enhancing lesions and iii) mixed or combined forms of lesions. Tuberculoma en plaque have been described to be located in frontal and parietal convexity, interhemispheric fissure, tentorium cerebelli and posterior fossa.3,4,7,8 Other CT findings including white matter edema and sulcal enhancement have also been described.3 The differential diagnosis includes meningioma, lymphoma, AVM, metastatic tumor, sarcoidosis and empyema, but these lesions are unlikely to produce the characteristic CT picture. Recently, Gd-DTPA enhanced MRI have been shown to be superior in cases of meningeal tuberculosis.2 Since medical therapy is generally effective for intracranial tuberculomas, increased familiarity with this form of tuberculomas can heighten the index of suspicion and thus prevent aggressive surgical resections which lead to increased mortality and morbidity. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02133f1.jpg] [ni02133t1.jpg] [ni02133f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}