 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 504-507 Case Report Scleroderma, Stroke, Optic Neuropathy : A Rare Association C.P. Das, S. Prabhakar, V. Lal, P.S. Kharbanda Department of Neurology,
Postgraduate Institute of Medical Education and Research,
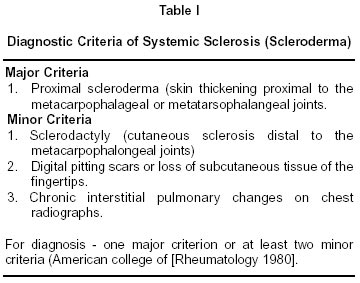
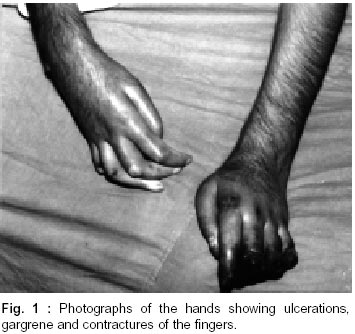
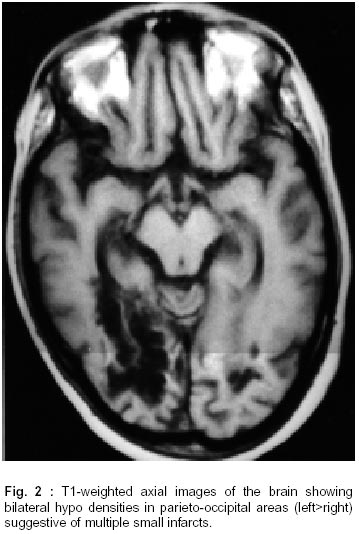
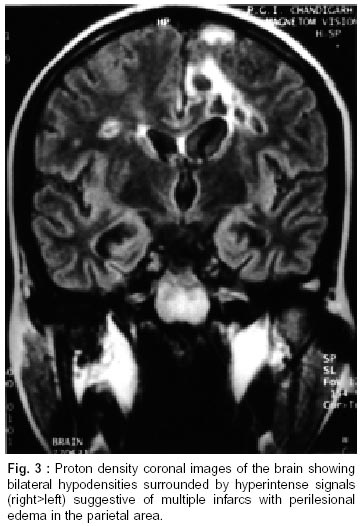
Chandigarh - 160 012, India. Accepted for publication : 2nd February, 2002. Code Number: ni02135 Summary A known case of scleroderma presented with right hemiparesis, focal seizures, optic atrophy and gangrene of digits. There was no evidence of peripheral nerve or muscle involvement. MRI showed multifocal infarcts in both cerebral hemispheres. MR angiography revealed poor flow in bilateral carotid arteries with collateralization from posterior circulation. She improved with phenytoin, nifedipine, antibiotics and immunosuppressants. The rarity of central nervous system affliction in scleroderma and large vessel vasculitis is discussed along with review of literature. Key words : Scleroderma, Stroke, Neurologic manifestation. Introduction The term 'scleroderma' refers to a group of disorders that share the common feature of thickening (sclerosis) of the skin. Although the cutaneous manifestations are the most striking, generalized scleroderma is a systemic disorder that can affect virtually any organ system and is more appropriately referred to as 'systemic sclerosis'. The pathology of different organ system involvement was first demonstrated by Goetz.1 The American college of Rheumatology has laid down the diagnostic criteria (Table I) for systemic sclerosis.2 Certain medical diseases, and disorders in response to environmental, mental or extrinsic factors may result in a scleroderma like syndrome and are termed as secondary scleroderma. Rarely systemic sclerosis may not have skin changes ('systemic sclerosis sine scleroderma'), or may coexist with other connective tissue disorders e.g. systemic lupus erythematosis, polymyositis etc. ('overlap syndrome'). Lungs, kidney, gastrointestinal tract, joints and the heart are the common organ involvement in scleroderma besides the skin. Cerebrovascular ischemia is very rarely seen in patients of scleroderma.3 Scleroderma 'per se' is a rare disease with an incidence of 0.1-14 per 100,000 of general population. It is the rare manifestation of a rare disease that has prompted us to report this case. Case Report A 19 years female was admitted with acute onset right sided hemiparesis and poor speech output 8 months earlier and progressively decreasing vision of both eyes (left>right) over 2-3 months, 6 months back. She developed blackening and ulcerations of her fingers and fever one month prior to admission. Her immediate problem was recurrent focal seizures of face (right side) and right upper limb. She had already been diagnosed as scleroderma two years back (October 1998) and was on dexamethasone 30 mg once daily. She had also received cyclophosphamide for 6 months which was discontinued because of development of anemia. She was non-diabetic, nonhypertensive and did not complain of breathlessness, palpitation, dysphagia or malabsorption. There were no sensory complaints, loss of consciousness, cognitive decline or sphincter abnormalities. Examination revealed a pale lady with difficult to palpate peripheral pulses. The carotid and femoral pulsations were also feeble. She had thick skin with a pinched nose and restricted mouth opening. There were sloughing ulcers over the knees and elbows with contractures and gangrenous changes over her fingers (Fig. 1). The respiratory, cardiovascular and abdominal examination did not reveal any abnormality. She had a depressed mood and could count fingers at one metre. Fundus examination showed optic atrophy. Other cranial nerves were normal. There was a right sided spastic, hyper-reflexic hemiparesis (3/5 power by the MRC scale), along with epilepsia partialis continua involving the right eye, angle of mouth and upper limb. Right plantar was extensor and the abdominal reflexes on the same side could not be elicited. All sensations were preserved. There were no cerebellar signs. Investigations revealed Hb - 10.7 gm/dl, TLC - 6000/Cmm (N72L20M6E2), ESR (1st hour) - 26 mm and platelets - 2.79x105/cmm. Serum Na+/K+ (134/3.8 meq/L), urea/creat (45/0.5 mg/dl), albumin/globulin (4.2/3.5 gm/dl) and liver function tests were normal. She had a strongly positive ANF (+++), but her LE cell, rheumatoid factor (RF) and antiphospholipid antibodies were negative. Fever work up, inclusive of blood/urine culture, 'widal test', blood for malarial parasite, chest X-ray, echocardiography and abdominal sonography were non-productive. Skin biopsy showed focal extension of dermal collagen into the subcutaneous tissue, and was consistent with scleroderma. CPK value, electromyography and nerve conduction studies were within normal limits. Visual evoked potentials of both eyes were not recordable. The MRI Showed multifocal areas of infarct (Fig. 2 and 3) involving bilateral parieto-occipital, left frontal and right temporal cortex. MR angiography showed small caliber and poor flow of both internal carotids and collateralisation of the anterior circulation from the vertebral and basilar arteries. The patient was started on phenytoin 600 mg for 2 days followed by 300 mg daily, and her focal seizures subsided completely within 5 days. Her finger ulcerations and gangrene improved with conservative management, thereby avoiding amputation. She was discharged on prednisolone 15 mg daily with monthly doses (500 mg) of IV cyclophosphamide. At 6 months follow up her hemiparesis had improved (4+/5) and she could count fingers at 2 m, however the contractures of her fingers had worsened. Discussion Neurological complications of systemic sclerosis were considered rare and thought to be coincidental, iatrogenic or secondary to involvement of other organs like kidney or gut, rather than due to the disease itself.4 Over the past decade, studies which included subclinical muscle involvement have shown a much higher incidence (upto 40%) of neurological involvement.3,5,6 Patients with anti-U1 RNP antibodies, and anti-ScI-70 antibodies are at higher risk of developing neurological complications.7 Myopathy is the commonest form of neurologic manifestation in scleroderma. In patients followed up for long periods and examined with manual strength testing, electromyography, muscle enzyme levels and muscle biopsy, upto 96% of cases showed some form of muscle involvement.8 However, documented muscle weakness and disease corroboration by an abnormal muscle biopsy was reported in only 7% of cases.4 Systemic sclerosis typically precedes muscle involvement by several years.3 The present case did not have any muscle weakness. Her right hemiparesis was due to a central cause. She had a normal CPK and electromyogram. Since the duration of disease was only 2 years it is possible that she has not yet developed a myopathy. Peripheral neuropathy is seen in 10-20% patients of scleroderma.3 Distal axonal polyneuropathy is the commonest. The exact pathogenesis is uncertain but usually does not involve vasculitis. Ischemic infarction of different nerves may result in a painful mononeuropathy multiplex. The peroneal nerve in the lower limb and ulnar nerve in the upper limb is the commonest to be involved. Unilateral or bilateral optic neuropathy has also been seen in scleroderma.6,9,10 The present case had bilateral optic neuropathy as evidenced by optic atrophy on fundoscopy and unrecordable visual evoked potentials. The peripheral nerves of the extremities were however normal, both clinically and electrophysiologically. Central nervous system involvement is rare in scleroderma, possibly due to the paucity of connective tissue and lack of an external elastic lamina with a sparse media and adventitia of cerebral arteries. When it occurs, cerebral ischemia is generally associated with evidence of renal failure or hypertension.4,11 Hemiparesis and transient ischemic attacks have been seen in only 2-6% of cases.3,5 There has been a report of transient global amnesia possibly as a result of 'Raynaud's phenomenon-like' cerebral vasospasm.12 Localized scleroderma of .the scalp associated with focal stenosis of the M2 portion of middle cerebral artery (R) has also been reported.13 Another angiographic study demonstrated symmetrical segmental narrowing of the superior cerebellar arteries, with filling up of the posterior cerebral arteries from the carotid territory.14 The 45 year old patient was hypertensive and also had 50% stenosis of left common carotid. By contrast our patient was young (19 years) non-hypertensive and had a normal lipid profile. Her both the carotid arteries were narrow and it was the posterior circulation that sent out rich collaterals. Since her antiphospholipid antibody was negative and no other cause for arterial narrowing could be ascertained, it was possibly related to scleroderma induced vasculitis. Other rare CNS abnormalities described include encephalopathy, sub-arachnoid hemorrhage, psychosis and anxiety disorder.l4-16 Treatment with corticosteroids or cyclophosphamide have been found to be beneficial as occurred in our case. Seizures can occur as a result of vasculitis or as a complication of the 'en coup de sabre' of linear scleroderma, wherein band-like sclerosis of the leptomeninges and associated vessels may occur with calcified and anomalous vessels in the underlying parenchyma.17 Similar to other rheumatologic disease e.g. rheumatoid arthritis, a sparing effect of the primary disease on the hemiparetic side has been described in scleroderma.18 In the present case also the gangrene and ulcerations were more severe on the healthy (left) side (Fig. 1). On follow up, the contractures were also prominent on the left hand / fingers. The exact cause of this phenomenon is not known. Anecdotal reports have shown development of myasthenia gravis either before or after diagnosis of systemic sclerosis.3,4 This may be a chance association or due to the presence of HLA B8/DR3 predisposing to both diseases. Myelopathy with spastic quadriparesis has also been associated with scleroderma. Although concomitant gastrointestinal tract affliction was detected the patients had normal vitamin B12 andVitamin E levels, and no evidence of cerebrospinal pleocytosis. Hence no reasonable explanation other than scleroderma was found. In the present case, the patient did not have hypertension or renal involvement which are commonly associated in the rare event of scleroderma induced central nervous system involvement. However, since we do not have any alternative explanation the possibility of large vessel vasculitis secondary to scleroderma remains high. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02135t1.jpg] [ni02135f3.jpg] [ni02135f1.jpg] [ni02135f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}