 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 511-513 Aneurysmal Bone Cyst of the Temporal Bone - A Case Report D. Purohit, S. Chopra, V.D. Sinha, S.R. Dharker Department of Neurosurgery,
S.M.S. Medical College,
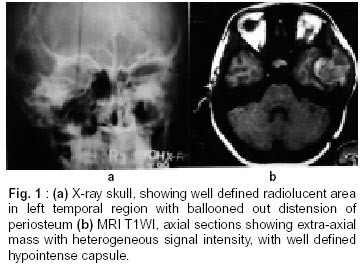
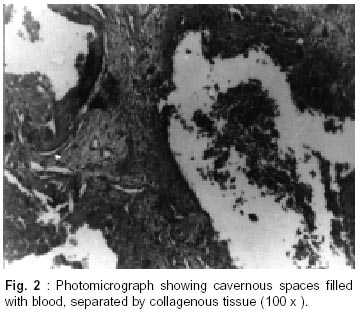
Jaipur - 302 004, India. Accepted for publication : 18th December, 2000. Code Number: ni02137 Summary Aneurysmal bone cyst in temporal region is rare. It is a benign condition and may extend intracranially. Total surgical removal is recommended, whenever possible in one stage or in multiple stages. Prognosis is excellent and total removal will effect a cure. An unusual case of aneurysmal bone cyst of temporal region is reported. Key words : Aneurysmal bone cyst, Benign neoplasm, Ballooned out distension. Introduction Aneurysmal bone cyst is a rare and benign lesion of the skull with obscure pathogenesis.1 Approximately, 36 to 50% of all aneurysmal bone cysts are found near one end of long bone and 25% involve the vertebrae, hyoid, mandible and odontoid.2,3 The reported incidence in the skull is 1% of all aneurysmal bone cysts.4 Sixty three cases of aneurysmal bone cysts of skull have been reported in the literature, of which 11 were of temporal bone.5 An unusual case of aneurysmal bone cyst in the left temporal region is reported here. Case Report A 13 year old girl was admitted with gradually increasing painless swelling in the left temporozygomatic region for last 3 months. She had pain off and on in the swelling for the last one month. There was no history of trauma. On examination there was a non-tender mass, 7x5x3 cm in size, in the left temporozygomatic region; which was firm to hard and fixed to bone with smooth surface. Skin over the swelling was normal. There was no neurological deficit. All routine investigations were within normal limits. X-ray skull revealed a round well defined radioluscent area in the left temporal region with ballooned out distension of periosteum outlined by a paper thin subperiosteal bone. There was also erosion of greater wing of sphenoid (Fig. 1a). CT scan head (plain and enhanced) showed extra axial hetrogeneous mixed density mass in the left temporal region, taking irregular variegated enhancement. The mass showed medial extension compressing left temporal lobe. There was erosion of petrous and sphenoid wing of temporal bone. MRI showed large well defined extra axial mass lesion with heterogeneous signal intensity in the left temporal and infratemporal region on T1 weighted. The mass showed medial extension with compression of temporal lobe. The mass had well defined hypointense capsule (Fig. 1b). On T2WI, the above described lesion showed homogenous increase in signal intensity. A left temporal question mark skin flap was raised with temporalis muscle. The underlined temporal bone was thinned out with erosion of petrous and greater wing of sphenoid. The tumor had well defined capsule and was soft in consistency. Dark coloured blood was aspirated from the cyst. Near total excision of cyst was done. The squamous part of temporal bone was thinned out and temporal dura was adherent to it, which was torn during tumor removal. Dural defect was repaired by pericranial patch. Inferiorly, tumor mass was extending upto the floor of middle cranial fossa and posteriorly to the petrous bone. Near total excision of the tumor was done. Radiotherapy was not given. The patient was symptom free in the post operative period after 7 months of surgery and kept under close follow up. Histopathological examination showed cavernous spaces filled with blood. The spaces did not show any endothelial lining. Large areas of extravasated blood were seen. The spaces were separated by collagenous tissue containing fibroblasts, focal collections of osteoclastic and intermediate giant cells. Normal bony trabeculae being permeated by the lesion seen in the periphery was suggestive of aneurysmal bone cyst (Fig. 2). Discussion The incidence of aneurysmal bone cyst in the skull varies from 3 to 6% of all aneurysm bone cysts.6-9 They usually present as scalp mass.6,7,10,11 Occasionally, they may present as intracranial space occupying lesion12 or cerebral hemorrhage.13 Age of presentation varies, but they usually present in the second or third decade, with equal sex distribution.4,5 In 1942, Jaffe and Lichtenstein14 introduced the concept of aneurysmal bone cyst as a lesion with characteristic radiological appearance of ballooned out distension of the periosteum, usually outlined by a paper thin subperiosteal bone shell which is overlined by a region of disintegrated cortex. Trauma has been put forward as an important etiological factor.15,16 Edling1 regarded aneurysmal bone cyst as one of the manifestation of solitary dysfibroplasia of bone, suggesting a defect in development of the epiphyseal plate but it does not explain its occurrence in the mature bone. Lichtenstein2 suggested that it could result from local circulatory disturbance, because of sudden vascular occlusion of venous drainage of that segment of bone or development of an arterio-venous shunt. This results in progressive blood spaces in the medulla, which lead to gradual distension of the bone with atrophy. Jaffe17 reported that a pre-existing lesion of bone may initiate an osseous A-V fistula. Aneurysmal bone cyst in coexistence with other lesions of bone have been reported3,18,19 and include unicameral bone cyst, non-ossifying fibroma, gaint cell tumor, chondroblastoma, fibrous dysplasia, osteofibrous dysplasia of campanacci, fibrous histiocytoma osteoblastoma and cartilaginous hematoma of chest wall of infants. CT scan is superior to plain radiology in defining extent and soft tissue extension of an aneurysmal bone cyst, particularly in the skull. Multiple small fluid levels are important characteristics of aneurysmal bone cyst on CT scan, which represents sedimentation of red blood cells within blood filled cavities.20 The aneurysmal bone cysts which do not show fluid levels on CT scan are often non-homogeneous and resemble some giant cell tumor,20 also seen in the present case. MRI also shows fluid levels, particularly in TlWI. Other findings include prolonged relaxation time, complete delineation of the margin of the lesion by a rim of low intensity signal and internal septation creating cystic cavities where wall contains diverticulum like projections.21 In our case, multiple fluid levels were not seen. Parikh et al4 also did not find fluid level in their case. Pathologically, these cysts contain multiple fluid filled cavities separated by multiple septa lined by mutinucleated giant cells. These large spaces filled with blood do not have an endothelial lining, but are rather delimited by cells with the morphology, ultrastructural and immunohistochemical features of fibroblasts, myofibroblasts and histiocytes. Aneurysmal additional feature of a peculiar degenerated calcifying fibromyxoid tissue reported by Rosai.19 The risk of recurrence is increased with an increase of mitotic figures.22 In some cases, surgical biopsy has in itself been curative.23 Total excision has been recommended as an ideal treatment for aneurysmal cyst of skull.18 Simple curettage is associated with high recurrence rates varying from 21% to 50%.13 The tendency for recurrence is related with young age of the patient, size of the lesion, presence of mitosis and incomplete surgical removal. Radiotherapy has been advocated for deeply situated lesions of the base of the skull, dural involvement or where subtotal excision is done but its effect is unclear.13,24 The suggested dose ranges from 600 to 3000 rads.18,25 Radiotherapy is however contraindicated in the treatment of aneurysmal bone cyst associated with fibrous dysplasia as there are increased chances of malignant transformation.26 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02137f1.jpg] [ni02137f2.jpg] |
| |||||||||

{kind=link}
{kind=link}