 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
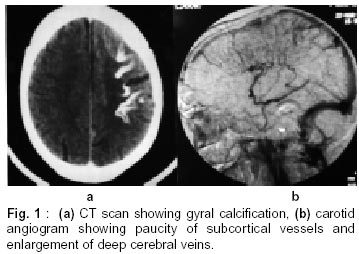
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 522-523 Short Report A Case of Hemeplegic Migraine with Leptomeningeal Angiomatosis A.S. Girija, V. Somanath Correspondence to : Dr. A.S. Girija, Professor, Department of Neurology, Medical College, Kozhikode - 673 008, Kerala India. Code Number: ni02142 Summary A 43 year old man with thirty years history of recurrent hemiplegic migraine, consistently occurring on one side (left sided paresthesia and weakness of less than forty five minutes followed by right sided headache) and lately increasing to once in three days was investigated. CT head and carotid angiogram showed gyral calcification with prominent medullary and subependymal veins confirming the diagnosis of leptomeningeal angiomatosis. Management and followup is discussed. Key words : Gyral calcification, Hemeplegic migraine, Migraine prophylaxis. Introduction Leptomeningeal angiomatosis is associated with a variety of skin manifestations including angioma of face, neurofibromatosis type 2,1 and hair follicle nevus.2 It has also been reported sporadically. The commonest clinical manifestation is epilepsy with or without hemiparesis. Hemeplegic migraine as a presenting feature is extremely rare. A case of facial angioma with hemiplegic migraine due to focal chronic ischemia proved by PET studies but without definite leptomeningeal angiomatosis and responding to aspirin is on record.3 The present case is noteworthy for its absence of neurocutaneous markers, presentation solely as hemeplegic migraine with leptomeningeal angiomatosis and the futility of common anti migraine drugs. Case Report A 43 year old man was admitted with 30 year history of recurrent attacks of hemeplegic migraine. This starts as paraesthesia over the left half of the body lasting for 15 minutes followed by left sided weakness. The weakness and numbness lasted for 30- 45 minutes and he developed throbbing headache in the right temporal region which resolves by 4 to 6 hours. There was no loss of consciousness, vomiting, seizures, photophobia or phonophobia. These episodes used to occur once in six months in the early years but had increased in frequency to once in two to three days and were disabling. There was no definite precipitating factors. There was no family history. He was a chronic heavy smoker. Clinical examination revealed no neurocutaneous markers. Ocular fundi were normal. There was no neurological deficit. Investigations : Urine - normal, Hb - 14.3 gm%, PCV - 44%. Platelet count - 2.21 lakhs/ mm.3 Blood sugar, BUN, serum creatinine, ECG, X-ray chest and ultra sound scan of abdomen, and EEG were normal. Xray skull showed gyral calcification in the right frontoparietal region. A four vessel cerebral angiogram was also done which showed paucity of vessels in the right frontoparietal area during venous phase with prominent medullary and subependymal veins confirming the diagnosis of leptomeningeal angiomatosis and also excluded associated arteriovenous malformation. He was initially started on propranalol (120 mg/ day) and flunarizine (10 mg) without any benefit after three months. He could not tolerate higher doses of propranalol and even increase in the dose of flunarazine to 15 mg was not helpful. The patient was then started on carbamazepine 200 twice a day. He was asymptomatic for the next eight months except for an occasional mild paresthesia. However, while on this drug he was admitted with left sided weakness, headache and loss of consciousness, of four hours duration which had never occurred eariier. Examination revealed a stuporous patient without neck stiffness. He had a gaze paresis to left. Ocular fundus was normal. There was weakness of limbs more on left side and the plantars were extensor. There was incontinence of urine. A repeat CT head scan did not show any new abnormality. EEG showed 'bipleds' in the frontotemporal and parietal regions. The patient remained stuporous for more than 36 hours, after which he spontaneously recovered. The EEG became normal. He was put on divalproex sodium 300 mg twice a day and is on follow-up. There has been no recurrence of any symptoms for over an year. Discussion This patient had classical hemeplegic migraine consistently occurring on one side without any family history and increasingly disabling with advancing age which prompted extensive investigations. Gyral calcification has been reported in leptomeningeal angiomatosis associated with Sturge Weber Dimitri syndrome and recently in Coeliac disease.4 This patient however had no facial angioma, angioma in ocular fundus, raised ocular tension, epilepsy or hemeplegia which constitute the former, or any gastrointestinal symptoms with epilepsy which can coexist with Coeliac disease. CT with contrast study confirmed the diagnosis of leptomeningeal angiomatosis. Cerebral angiogram in addition excluded any arterovenous malformation and showed paucity of vessels in the right frontoparietal region. MRI with contrast offers additional advantage in the diagnosis of leptomeningeal angiomatosis by showing ischemic changes affecting grey and white matter and the cranial diploeic prominence on the affected side.5 MRI was not done in this case as there was enough evidence for leptomeningeal angiomatosis with CT and carotid angiogram. Beta blockers (120 mg/day) along with flunarizine 15 mg/day had no effect at all either in frequency or severity of attacks the cerebral. The case reported by Cambon et al3 which has the nearest resemblance to the present case, responded to aspirin. In this case, there was regional oligemia demonstrated by PET studies. The authors considered this as an atypical case of Sturge Weber syndrome though he had only hemeplegic migraine with facial angioma and interhemespheric asymmetry without any leptomeningeal angiomatosis. The case under discussion did not respond to flunarizine and he was started next on carbamazepine, considering the high association of epilepsy and leptomeningeal angiomatosis. EEG also supported wide spread functional disturbance as evidenced by 'bipleds' in the fronto temporal region when he became unconsious. PLEDs in EEG are indicative of subacute neuronal injury. However, this type of EEG abnormality has not been described in migraine. The evolution of the symptoms, the duration, and the complete recovery are suggestive of a vascular etiology. The response to sodium valproate and carbamazepine, rather than to betablockers, flunarizine, may suggest a neuronal excitation process as in epileptogenesis preceding a vascular phenomenon as the cause of the symptom. 'Cephalgic seizure' described earlier differs from the case described in the absence of aura and hence in the abruptness of onset of headache and occurrence in the pediatric age group.6,7 The patient had been on Carbamazepine 200 mg twice a day along with Divalproex sodium for over one year without any headache or aura. Attempts on reduction of Carbamazepine worsened the situation and hence he was continued on both the drugs. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02142f1.jpg] |
| |||||||||

{kind=link}