 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
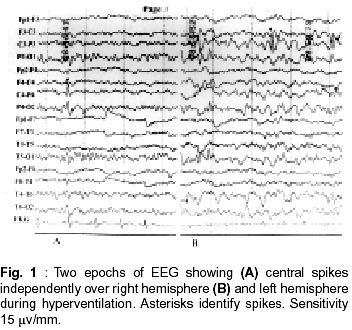
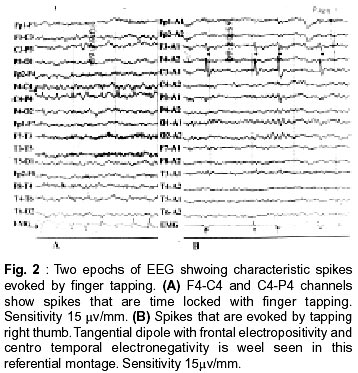
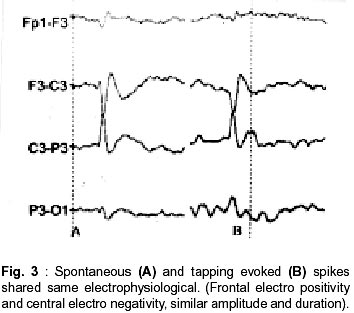
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 524-525 Short Report Finger Tapping Activates Spikes in Benign Epilepsy with Centro-Temporal Spikes P. Rajesh, K.P. Vinayan, S.V. Thomas Correspondence to : Dr. S.V. Thomas, Department of Neurology, Sree Chitra Tirunal Institute of Medical Sciences and Technology, Trivandrum - 695 011, India. Code Number: ni02143 Summary A case of benign epilepsy with centro-temporal spikes (BECT) is reported, in whom tapping of fingures activated typical spikes. Key words : Spike and waves, Benign epilepsy. Introduction Benign epilepsy with centro temporal spikes (BECT) constitutes over six per cent of all non-febrile epilepsies in children and undergoes spontaneous remission in most children before the age of 18 years.1 Incomplete semiological description and inadequate EEG evaluation are the common reasons for under reporting of this disorder with good prognosis. EEG is most helpful when it shows typical spike and wave discharges over centro - temporal region. Shifting foci and normal background activity are the two EEG characteristics of BECT in contrast to fixed focus and abnormal background activity observed in symptomatic focal epilepsies. Recently it had been observed that the spikes in BECT could be activated in a time locked manner by electrical stimulation of the digits or by tapping on the tendons.3 Tapping on the tendon is a simple technique that can be applied in any standard laboratory. We report a case of BECT where in tapping the fingers could activate typical spikes. Case Report A 7 year old girl was referred to the EEG services for the classification of her seizures. She was the firstborn child of a consanguineous marriage with normal birth and development and no history of febrile seizures. There was no family history of febrile seizures, epilepsy or any other neurological illness. She had three episodes of seizures within a span of two months characterized by paresthesia over tongue and lips followed by chattering of teeth, speech arrest, salivation and tonic clonic movements of right upper limb. Seizure used to last for about 30 seconds to one minute. Child was well aware of the attacks. She did not have any post-ictal paresis or confusion. She was not on any medication at the time of EEG. Examination revealed no neurological deficits including soft neurological signs. Neuroimaging was not done. EEG description : EEG was recorded for about forty minutes in awake state. There was no sleep record, as the patient did not sleep naturally or with triclofos. The activation procedure consisted of gentle tapping on the volar aspect of thumb or other fingers with a tendon hammer. The taps were delivered at random or regular interval (approximately 1-2/sec). An EMG channel was used as an event marker with surface EMG electrodes placed at the root and tip of each fingers. Results The background activity of the awake record consisted of 9-10 Hz alpha rhythm over the posterior head regions, that was bilaterally symmetric and synchronous, attenuating to eye opening and mental alerting. Intermittently bilateral independent central spikes were observed with phase reversal at C3 or C4. In ipsilateral earlobe reference montage, a clear tangential dipole was seen independently over both sides (Fig. 1). Tapping on the fingers consistently evoked spikes over the contra-lateral central area with tangential dipole (Fig. 2). Evoked spikes had same morphology as spontaneous spikes (Fig. 3). It was observed that the spikes elicited (by finger tapping) had higher amplitude over the left central region compared to the right central region. In addition, the spikes had better definition, amplitude and wider spatial distribution (field extending to temporal area) when the thumb or lateral 2 digits were tapped. There was no spread to temporal area while tapping on the medial 2 fingers. Tapping any of the five fingers on right hand evoked spikes over the left central area, where as tapping the lateral four fingers of the left hand only evoked spikes over right central area. All the evoked spikes on the right side were strictly confined to central area. Discussion The girl under discussion has presented with fairly typical history of BECT. The EEG confirmed the diagnosis. This case demonstrates the usefulness of EEG activation procedure in reaching a precise diagnosis. Ajmone and Zivin observed that about 55%of patients with epilepsy might show epileptiform activity in the first awake examination.4 Later Binnie showed that a combination of awake and sleep record would bring out epileptiform discharges in about 80% cases of epilepsy.5 Activation procedures like hyperventilation, photic stimulation etc. increase the yield of EEG in epilepsy patients. However, a single procedure may not be effective in all types of epilepsies, e.g. hyperventilation is very helpful with absences but not so helpful with juvenile myoclonic epilepsy, which shows high incidence of photic activation. These procedures have not been very helpful with BECT.2 Finger tapping is a simple procedure that has recently been reported to activate epileptiform activity in BECT.3 They had demonstrated that the spontaneous spikes and elicited spikes had same morphology. We had followed a similar technique that consistently evoked spikes over contra lateral central area. The evoked spikes also had the typical tangential dipole and other morphological characteristics of spikes of BECT as observed by Manganotti. However unlike his observation, spikes could be elicited by tapping any of the fingers on right hand or lateral four fingers on left hand. In this study, tapping all fingers on the right and lateral 4 on the left hand evoked spikes. Activation of spikes with finger tapping has not been described with any other condition so far. With finger tapping activation, it was possible to bring-out the silent focus on the other hemisphere. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02143f3.jpg] [ni02143f2.jpg] [ni02143f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}