 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
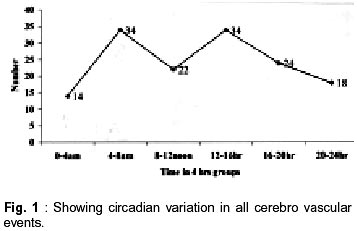
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 526-527 Short Report Circadian Pattern in Cerebro Vascular Disorders A. Bhalla, R. Singh, A. Sachdev, S. D'Cruz, A. Duseja Correspondence to : Dr. A. Bhalla, Govt. Medical College, House No. 1032, Sector - 24/B, Chandigarh - 160 023, India. Code Number: ni02144 Summary Over the last decade, various studies have been reported to evaluate the circadian pattern of cardiovascular and cerebro-vascular diseases. The data from Indian population is lacking. We undertook this prospective observational study to evaluate the circadian variation in disorders like cerebro-vascular accidents and transient ischemic attacks. Total of 146 patients (events) were studied. Only 10 patients had TIA's. 55% had hemorrhage and 45% had infarction. The 24 hours period was divided into 6 equal portions of 4 hours each. The maximum events were seen between 4 am to 8 am and 12 noon to 4 pm (23.28%) each. Minimum events were seen between 12 midnight to 4 am 14/146 - 9.58%). The circadian variation in occurrence of cerebro-vascular disorders was present with two equal peaks. Key words : Circadian variation, Cerebrovascular events, Stroke. Introduction A land mark study by Pell and D'Alanzo described the presence of circadian variation in occurrence of myocardial infarction for the first time in 1963.1 In the last thirteen years it has been consistently shown that there is an increase in cardiovascular and cerebrovascular event rate during the early morning hours. Presence of circadian variation is reported in blood pressure, ventricular rate, refractoriness of the ventricle, anginal attacks and sudden cardiac death.2,3 The rise is more marked during the early morning hours, immediately after getting up from sleep.2,4,5 This study was undertaken to find the existence of circadian variation in cerebro-vascular events, in urban population in and around Chandigarh. Material and Methods All the patients attending emergency services of Government Medical College Chandigarh, with complaints suggestive of cerebro-vascular disease were included. The patients / relatives were asked about the time of occurrence of first symptom and time of subsequent episodes were also noted. Clinical examination and CT scan were done to establish the diagnosis of acute cerebro-vascular accident. The patients with diagnosis of TIA were examined to rule out cardiovascular diseases and observed for progression of symptoms. The day was divided into 6 equal periods of 4 hour each. The data was analyzed by using EPI 6 statistical package as percentage of events occurring during specific time interval. Results A total of 146 patients (events) were studied. 64.2% patients were males and 35.8% were females. The mean age was of 58.5 ±6.5 years. 55% patients had hemorrhagic stroke 45% had ischemic stroke. Only 10 patients had transient ischemic attack (TIA's). Since the number of patients with TIA's was very small for analysis all CNS events were considered together. The 24 hour day was divided into 6 equal parts each. Maximum events were seen during the period between 4 am to 8 am (34/146) and between 12 noon to 4 pm 34/146. The least number of episodes were seen during the period between 12 midnight to 4am 14/146 (9.58%). The results were analyzed as percentage of the patients (events) occurring during the specified time period. Since the number of patients was small we did not divide the patients into various age groups for further subgroup analysis. Discussion The complex interplay between the protective and trigger factors is responsible for circadian variation. It is noted that these events do take place at other times during the day but at a relatively lesser rate than morning hours.2,5-7 Various physiological changes occur during the early morning hours as we get up and attain an upright posture. These changes can be grouped into hemodynamic changes, vascular changes and hematorrheologic changes.5,8 The most important haemodynamic change is the rise in heart rate and blood pressure. Along with decreased vagal tone, rise in catecholamine level and activation of renin angiotensin system, make the atherosclerotic plaque more liable to rupture and thrombosis.5,8,9 The vascular changes like increased vascular receptor sensitivity, increased vascular tone also contribute to the damage.2,8 Hematorrheologic changes like increased platelet aggregability on assuming upright posture, increased blood viscosity and a fall in the fibrinolytic activity, add fuel to the fire.2,6,8,10,11These factors alone are not capable of resulting in adverse events. Various trigger factors have been identified, which act in conjunction with physiological changes in the early morning hours.4,5,7,9 These factors are start of activity, bursts of anger, sexual activity and heavy physical exertion.4,5 These trigger factors can precipitate an acute attack at any time of the day. A shift in the time of awakening in the morning or getting up late and starting activity at a later hour does not negate the physiological effect of these factors but shifts to a later hour.12 Our study group showed the presence of circadian variation in cerebro-vascular events. The peaking of these events was noted twice, once in the early morning hours (4-8 am) and another similar peak between 12 noon and 4 pm. The minimum events were noted during 12 midnight and 4 am. Majority of the studies have been conducted with coronary events and a single morning peak has been noted for cardiac events like acute myocardial infarction and unstable angina. Some studies have been done in patients with stroke with similar results noted.3,13 Occasional studies in patients with coronary events have shown two peaks one in the early morning hours and another during the evening.10,14 The incidence of stroke for both ischemic and hemorrhagic strokes has been shown to be more during the hours between 8 am to 12 noon.13 In a study by Gur in which 599 patients of stroke were studied, 34% strokes occurred between 6 am and 10 am. No other parameter was found to be statistically different among the morning stroke patients compared to the strokes occurring at other times. However patients with arterial hypertension, ischemic heart disease and male patients had more likely hood of stroke between 10 pm and 2 am.15 In this study in the Indian population too the cerebro-vascular events follow the same pattern of circadian variation as indicated by some studies from the west. The reason for a morning peak has been elucidated in various studies but the evening peak can not be explained on the basis of physiological changes. The evening peak may be a result of trigger factors like stress, anger or other such factors. However further studies may be needed for looking into these factors. The importance of knowing these variations is in planning preventive strategies and planning dosing schedules for the patients.4 As two distinctive peaks are seen the preferred timing of scheduling dose would be after lunch to cover the evening peak between and another dose of long acting drug to be taken after dinner to cover the morning. In a recent study by Yosefy and colleagues from Israel it was found that long acting calcium channel blockers prevent the rise in blood pressure in morning hours and decreased incidence of stroke by around 50%; thus providing a comprehensive cover during the dangerous hours in the morning.16,17 The studies of these kind need to be done to plan and change treatment strategies. Larger studies from different parts of the country and from rural areas are needed for analyzing the presence of circadian variation amongst the different parts of our country and amongst different ethnic groups. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02144f1.jpg] |
| |||||||||

{kind=link}