 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
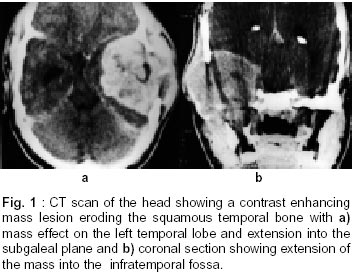
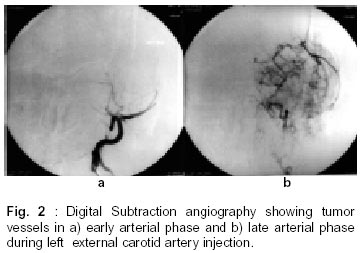
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 534-536 Short Report Skull Base Chondroblastoma : A Case Report R.K. Moorthy, R.T. Daniel, V. Rajshekhar, G. Chacko Correspondence to : Dr. V. Rajshekhar, Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632 004, India. Code Number: ni02148 Summary Chondroblastoma is a rare tumor of the skull. Temporal bone is the commonest site of involvement in the skull. We present a thirty one year old man who presented with painless swelling over the left temporal bone, which was near totally excised after preoperative embolization. Management of this unusual tumor and its complications are discussed. Key words: Chondroblastoma, Temporal bone, Embolisation, Infection. Introduction Chondroblastoma is a rare primary bone tumor accounting for about 1% of all primary bone tumors and it was first reported by Codman.1 The chondromatous nature of this tumour was confirmed by Jaffe and Lichtenstein.2 Commonly occurring in the epiphyses of long bones, skull is an unusual site for chondroblastoma. Of the few reported cases of skull chondroblastoma, the commonest site has been the temporal bone. The tumor has been known to have a benign course and complete excision has been the recommended treatment modality for chondroblastoma of the temporal bone.3-5,7,8,10 Case Report A 31 year old man presented with history of progressively increasing painless swelling over the left temporal region of nine months' duration. He had no focal neurologic deficits. A non-tender, bony hard swelling was palpable in the left temporal region with intact skin over it. There was no bruit. There was no regional lymph node enlargement. CT scan of the head showed a 6 x 7 x 6 cm hyperdense mass in the left middle cranial fossa which was eroding the petrous and squamous parts of the left temporal bone and extending into the subgaleal plane and into the infratemporal fossa (Fig.1). There was intense enhancement of the mass with contrast except in areas towards its centre, which were hypodense and nonenhancing. Digital subtraction angiography showed a very vascular tumor with feeder arteries from the left middle meningeal and maxillary arteries. There was no supply from the internal carotid artery (Fig. 2). He underwent preoperative embolization of the feeder vessels with gelfoam particles followed by near total excision of the mass. Intraoperatively there was a moderately vascular, firm, totally extradural mass that had eroded the squamous and petrous temporal bone and had infiltrated the temporalis muscle. It was adherent to the dura and was extending up to the foramen ovale also. The dura was not opened during the procedure. Postoperatively he developed left lower motor neuron type of facial paresis (Grade III House and Brackmann). On the second and third postoperative days he had serosanguinous discharge from the left ear. On the twelfth postoperative day he developed right hemiparesis and aphasia associated with fever, purulent discharge from the left ear and signs of meningeal irritation. CT scan showed evidence of subdural empyema, which needed drainage, initially through burrholes and later through a craniotomy. He was treated with long term antibiotics with which he made a good recovery. On follow up five months later, he was asymptomatic and had a left lower motor neuron type of facial paresis (Grade III) with no residual weakness of the right upper limb. He was then given conventional radiation therapy. Histopathological examination of the lesion showed a tumor with sheets of moderate sized polygonal cells with moderate amounts of eosinophilic and sometimes vacuolated cytoplasm with large rounded and often indented nuclei. Evenly dispersed amongst these cells were multinucleated giant cells. The stroma was spindle celled containing zones of chondroid material and few foci of 'chickenwire' calcification (Fig. 3). There wes sparse mitoses. The tissue sent during the re exploration also showed similar histopathology. Based on the above findings a diagnosis of chondroblastoma was made. Discussion Chondroblastoma is a rare primary bone tumor, which accounts for 1% of all primary bone tumors.3 It usually arises in the epiphysis of long bones with predilection for the upper end of humerus. Skull and facial bones are an extremely unusual site of occurrence. The squamous temporal bone is the commonest site of occurrence in the skull.5-7,12-14 There have been reports of involvement of the petrous temporal bone and extension into the adjoining middle cranial fossa, temporo-mandibular joint, skull base as well as the parotid region.7 Some authors have reported extension into the infratemporal fossa and parapharyngeal space, petrous temporal bone and middle ear cavity.9,13 The preponderance of occurrence in squamous temporal bone could be due to the fact that this portion of the temporal bone arises in cartilage. The common clinical manifestations reported are hearing impairment, tinnitus and ear stuffiness along with a swelling in the temporal region. Other symptoms include otalgia, seizures, vertigo and facial palsy.4,8,13-15 In the Mayo Clinic series of chondroblastomas of the skull and the facial bones, the mean age of presentation was 43.5 years.7 Our patient was in his thirties and he had presented with a bony swelling with no aural symptoms. Chondroblastoma of the temporal bone has been reported to have a fuzzily rarefied appearance and is sharply delimited from the surrounding bone by a thin margin of increased density.8 CT scan confirms the lytic nature of the lesion and shows areas of calcification. The main differential diagnoses include giant cell tumor, enchondroma and chondromyxoid fibroma.9 The radiological features of the lesion presented above are consistent with the findings described in earlier series. Codman's initial description of this tumor was as that of benign giant cell tumor of the chondromatous type.1 This was later reviewed and confirmed to be of chondromatous origin by Jaffe and Lichtenstein.2 The tumor characteristically has the polyhedral chondroblast, which is encased by reticulin. Pericellular calcification results in the 'chicken wire' calcification. The tumor has foci of chondroid production which appear pink and scattered osteoclast like giant cells. The presence of S100 immunopositivity in the tumor differentiates it from giant cell tumor, aneursymal bone cyst and chondromyxoid fibroma which are the main radiologic and pathologic differential diagnoses.7,8 Chondroblastomas are essentially considered to be benign, yet locally invasive and there have been very few reports of malignant chondroblastoma.10 Curettage with bone grafting is the treatment of choice for chondroblastomas of long bones. The lesion is then cauterised with phenol and treated with alcohol to devitalise the tumor cells that are left behind.11 Radical or total excision has been the recommended form of treatment for temporal bone chondroblastoma as local extension into middle ear, mastoid antrum and temporo-mandibular joint renders it difficult for curettage. In a review of literature by Narita et al quoted by Watanabe et al, recurrence rate after curettage was 43% while it was 27% after radical excision.7,12 Radiation therapy has been recommended only in cases of incomplete tumor removal. To the best of our knowledge, this is the first report where embolisation has been utilised to devascularise a chondroblastoma of the temporal bone prior to surgery. This facilitated near total excision of the tumor with minimal blood loss. There may have been partial rents in the dura during surgery that were not visualised and these might have resulted in the intradural spread of infection postoperatively. The residual tumor in the middle ear may have undergone necrosis secondary to the embolisation and could have been the nidus and route for infection. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02148f1.jpg] [ni02148f2.jpg] |
| |||||||||

{kind=link}
{kind=link}