 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
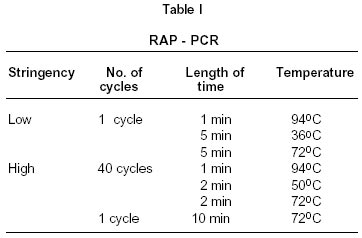
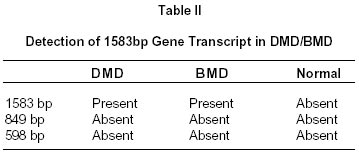
Neurology India, Vol. 50, No. 4, Dec, 2002, pp. 537-538 Short Report Detection of 1583 bp Gene Transcript in Lymphocytes of Muscular Dystrophy Patients S. Prabhakar, A. Anand Correspondence to : Dr. S. Prabhakar, Department of Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, Inida. Code Number: ni02149 Summary DMD and BMD are X-lined recessive disorders. RAP-PCR was utilized to investigate differentially expressed gene transcripts in lymphocytes from DMD, BMD and normal individuals as possible diagnostic parameter. A 1583 bp transcript was found to be expressed in both DMD and BMD patients which was unrelated to the known dystrophin gene. This may prove helpful in determining the carrier status of DMD/BMD. Key Words : Gene transcripts, DMD, BMD, RAP-PCR. Introduction DMD and BMD are X-linked muscular dystrophies, the former being fatal and the latter a milder variant. Mutations have been detected in the 2300 bp long dystrophin gene of these patients responsible for such diseased phenotype. The severity of disease is believed to depend upon the degree of deficiency of dystrophin, which is known to act in association with other sarcolemmal glycoproteins.1 Various methods like multiplex PCR, Southern analysis,2 direct sequencing, Western blot analysis,3 immunocytochemistry, CA repeat analysis,4 and single-strand conformations polymorphism have been successfully employed as diagnostic tools. Anand et al5 reported that DMD and BMD are allelic X-linked recessive disorders where three novel transcripts, i.e., 598bp, 849bp and 1583 bp are selectively expressed in patients of muscular dystrophy as compared to normal individuals. 598bp and 849bp transcripts were exclusively present in DMD patients and their families, but not in BMD. All these transcripts were reported to be completely unrelated to dystrophin gene. These studies were conducted exclusively in muscle biopsies. Due to the invasive nature of the procedure, an alternative and convenient means of possible diagnosis was explored by studying the expression of same transcripts in lymphocytes derived from blood. The patients who underwent routine muscle biopsies were subjected to lymphocyte based analysis of RAP-PCR products inorder to ascertain the presence of the these transcripts as diagnostic marker of the DMD/BMD. Methodology RNA isolation : About 5 ml of blood was drawn from patients and lymphocytes extracted. RNA from these lymphocytes of DMD, BMD and control subjects was isolated using TRI reagent (Sigma).It was quantified and checked for presence of contaminating DNA after DNAse I treatment. cDNA synthesis : About 100ng of RNA was used as starting template for cDNA synthesis. For this, about 1 µl of each arbitrary primer pair (AP) having the following sequence was used. A1 AATCTAGAGCTCCTCCTC, Following the incubation for 10 min at 70°C, the reaction was chilled on ice. About 1 µl of RNase inhibitor, 1 µl dNTP mix (25 mM each NTP), 2 µl of 10x first strand buffer, and 0.5 µl of MMLV - Reverse transcriptase (5 units/µl) were mixed and the contents incubated at 37°C for 1 hr to allow cDNA synthesis. RAP PCR : The PCR was performed using the same primer pair as used in cDNA synthesis. All reactions were performed in 50 µl reaction mixture containing 5 µl 10x Taq buffer, 3 µl 25 mM Mgcl2 (3 mM final concentration), 28.7 µl of distilled water, 0.2 µl of Taq polymerase, (5 U/µl), 2 µl of 25 mM A1 + A2 primers and 10 µl 1 : 10 diluted cDNA obtained from previous step. b actin RT PCR was performed as control reaction for normalization. The PCR cycles for RAPPCR and RT-PCR were as Table I. RAP-PCR products were visualized by running 6% polyacrylamide - 7 M urea sequencing gel. The gel was removed carefully and vacuum dried on gel drier at 85°C x 1½ hr. Subsequently, it was exposed to KODAK X-OMAT film for 3 days at -20oC. The film was developed and gel pattern obtained. RT PCR products were visualized in 3% agarose gel electrophoresis. Results and Discussion Post PCR analysis revealed the presence of 1583 bp gene transcript in patients of DMD/BMD (Table II). Further, in this study the RNA fingerprints obtained from the PCR were fewer than those obtained from muscle biopsies in the previous study by the authors This RAP-PCR study is conspicuous by the presence of 1583 bp gene transcript in the lymphocytes of DMD/BMD patients, which is along expected lines as reported by us in our study with muscle biopsies.5 This could be helpful in convenient diagnosis of muscular dystrophy patients and carriers by blood. This transcript is unrelated to dystrophin gene, known to be implicated in the pathogensis of muscular dystrophy. The expected DMD specific nature of the differentially expressed novel gene transcripts i.e, 849 and 598 bp is amply evident by their absence in the lymphocytes of DMD in the present study. This could be due to DMD specific expression of these transcripts in muscles only which is interestingly not reflected in blood. This could also be due to their decreased expression in lymphocytes as compared to muscles, the prominent site of pathogenesis. As an important aspect of developmental muscle biology the significance of local physiological dynamics governing the pathogenesis of DMD in muscle is reemphasised here in this report. The low expression of RNA fingerprints could be attributed to limited recognition of template by the given primer set. Utilization of another set of arbitrary primers could be a plausible alternative to further any diagnostic applicability of previously reported DMD specific novel transcripts in lymphocytes. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02149t2.jpg] [ni02149t1.jpg] [ni02149f1.jpg] |
| |||||||||

{kind=link}
{kind=link}