 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S2-S7 Stroke in India - Issues in Primary and Secondary Prevention P. M. Dalal Stroke Unit
and ICASS Research Cell,
Lilavati Hospital and LKMM Trust Research Centre,
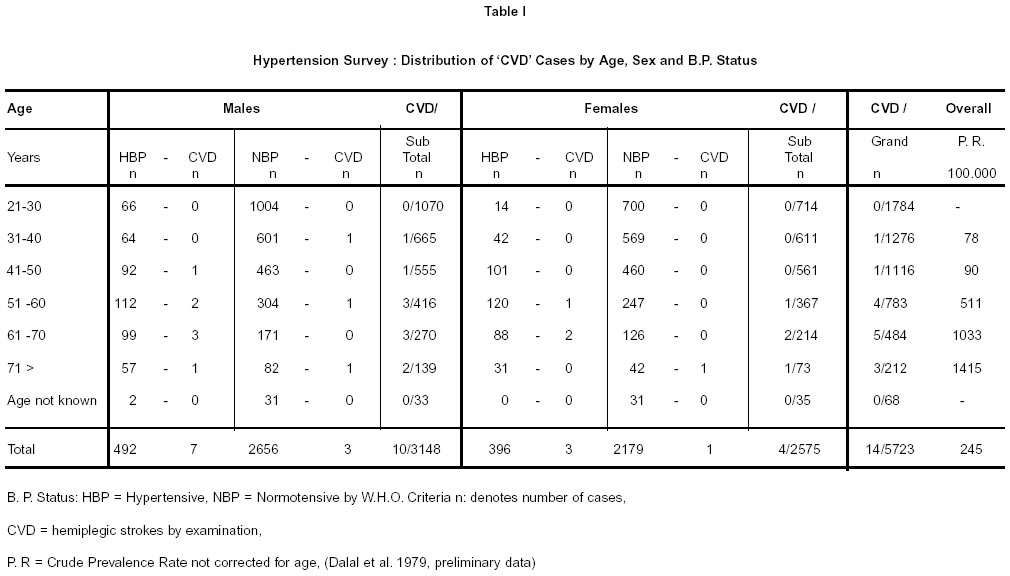
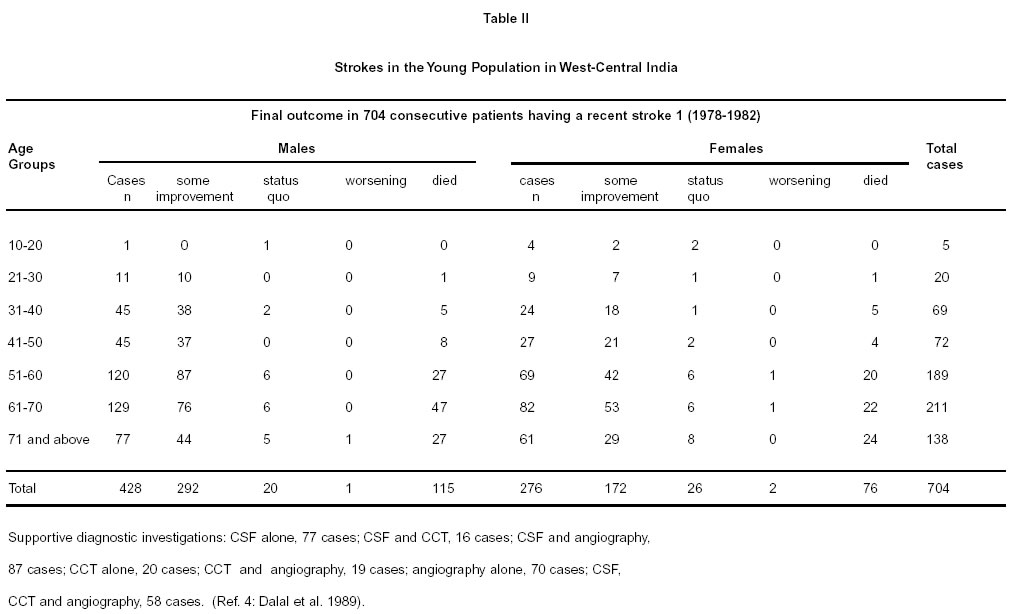
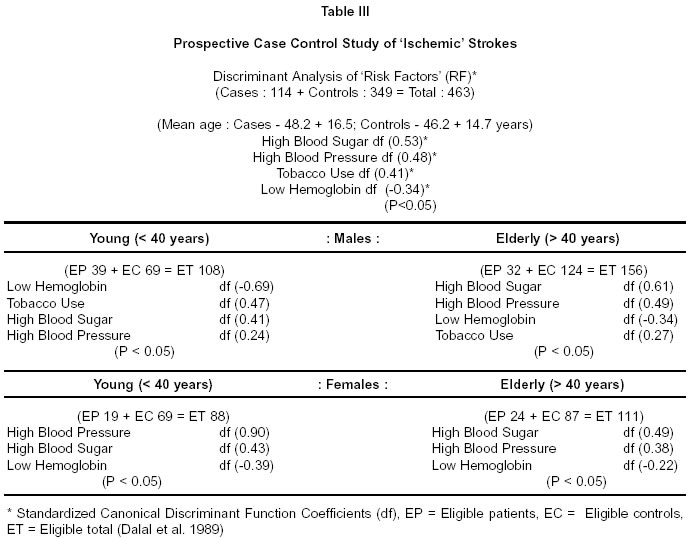
Ali Yavar Jung, Mumbai - 400 050, India. Code Number: ni02156 Summary India will face an enormous socio-economic burden to meet the costs of rehabilitation of stroke victims because the population is now surviving through peak years (age 55-65) of occurrence of stroke or cerebrovascular disease (CVD). Recent community surveys from many regions of India show a crude prevalence rate for strokes presumed to be of vascular origin in the range of 200 per 100,000 persons. Major risk factors identified in India are hypertension (> 95 mmHg diastolic), hyperglycemia, tobacco use (smoking/chewing) and low normal haemoglobin levels (< 10 gm%).A public awareness campaign focussing on the control of stroke risk factors, along with governmental support to implement a national health policy for screening high risk population in a cost effective manner, is highly recommended. Key words : Stroke, Prevention, India. Introduction India will face an enormous socio-economic burden to meet the costs of rehabilitation of stroke victims because the population is now surviving through peak years (age 55-65) of occurrence of stroke or cerebrovascular disease(CVD). However, for strokeprevention planning, reliable epidemiological information on annual incidence or prevalence rates and morbidity or mortality trends for CVD in defined populations are not available. Recent community surveys from many regions of India show a crude prevalence rate for strokes presumed to be of vascular origin in the range of 200 per 100,000 persons (Table 1),1 but there are numerous difficulties in validation of stroke diagnosis in these registries. Therefore, several prospective studies were initiated with well-defined protocols to identify etiopathology, risk factors (RFs) and morbidity / mortality trends at a community hospital in Mumbai, serving a nearby relatively stable populations. Material and Methods Terminologies as defined in the International Classification of Diseases have been adopted. Comprehensive designs of these studies, giving definitions, clinico-pathological correlations, pan-cerebral angiographic and necropsy findings, have been reported elsewhere.2-4 A stroke data bank has been established. All data have been encoded for future reference. Results Based on pan-cerebral angiographic and necropsy findings of the first study,2,3 it was possible to confirm that extracranial athero-lesions were chiefly responsible for thrombotic brain infarction, whereas intracranial lesions were documented in cerebral embolism cases; advancing age, hypertension and large cerebral infarcts carried grave prognoses. In an International Collaborative Study on the distribution of athero lesions, in 1090 circle of Willis (medicolegal and non medico- legal autopsies), it was found that athero-lesions began at an early age (<10years) and. severity of lesions progressed with advancing age, similar to what was reported in Minnesota (USA) and Fukuoka (Japan) centres.5 In the second prospective study in 704 consecutive patients having had a recent stroke, as verified by supportive / diagnostic tests, the general data by age and sex and survival status are shown in Table II.4 Comparing the two prospective CVD reports having identical methodologies and referral/observer bias, during the period 1963-68 and 1978-82, a significant drop was recorded in case fatality rate (32%-12%) thereby resulting in higher survival (68%-88%). These changing trends in morbidity/mortality patterns have now posed a major socio-economic challenge in rehabilitation of 'stroke-survivors'.4 In a subsequent multicentric prospective case-control study on risk factors in ischemic strokes, hypertension (> 95 mmHg diastolic), hyperglycemia, tobacco use (smoking / chewing) and low normal haemoglobin levels (< 10 gm%) were important risk factors (Table III).6-7 Concluding Remarks For India where its people are surviving through the peak years of stroke occurrence, preventive strategies are mandatory. Available data indicate that CVD occurs at all ages in both sexes and with increasing frequency in advancing age (Table I). From case-control data on risk factors, it appears that hypertension; diabetes mellitus, low normal haemoglobin and tobacco use (smoking / chewing) are important risk factors. Thus to design stroke prevention strategies, public awareness and health education on warning symptoms of hypertension and strokes by optimum use of existing mass media is vital. Life style changes, dietary habits and intensive campaign against tobacco use will prove rewarding. Primary health care teams should receive training on nomenclature and clinical diagnosis, in the absence of CT facilities in rural and remote areas. Mass screening surveys to identify 'hypertensives' and 'stroke - prone' subjects, wherever feasible, should be undertaken to prescribe simple, practical, non-costly remedies. The patients' compliance to clinic reference is usually unsatisfactory; hence, a cadre of medico-social/ multipurpose workers to remain in constant contact with such 'stroke-prone' individuals will have to be established to ensure regular intake of medicines and control of risk factors. National Councils to liaise between various agencies (health, industry, finance etc.) are essential to coordinate actions at all levels. The political will to legislate National Health Policy in support of above objectives is highly recommended.8-9 References
Suggested Reading Stroke Prevention (Secondary) General / Stroke mortality trends
Blood Pressure
Antiplatelet / Antithrombotic therapy in Stroke Prevention
Anticoagulant treatment
Neuroprotective Agents
Role of Surgery or Angioplasty in Carotid Stenosis
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02156t1.jpg] [ni02156t2.jpg] [ni02156t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}