 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S8-S14 Subtypes of Ischemic Stroke in a Metropolitan City of South India (One year data from a hospital based stroke registry) S. Kaul, P. Sunitha, A. Suvarna, A.K. Meena, M. Uma,* J.M. Reddy* Department of Neurology
and Imageology*,
Nizam's Institute of Medical Sciences,
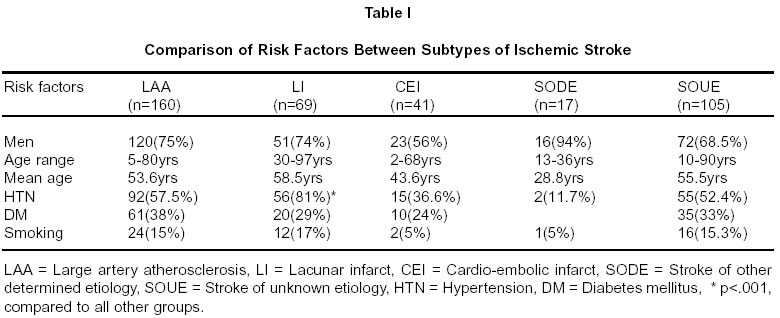
Hyderabad - 400 050, India. Code Number: ni02157 Summary Limited data exists on the subtypes of ischemic stroke from the Indian subcontinent. The present study was aimed to investigate the frequency, spectrum and risk factors of various subtypes of ischemic stroke in a south Indian referral center. The study was conducted on consecutive patients of ischemic stroke, fully investigated to determine the underlying mechanism and enrolled in the stroke registry of Nizam's Institute of Medical Sciences between Ist February 2000 to 31st January 2001. There were 282 men and 110 women (mean age 54 years; range 2-97 years). Of all ischemic stroke patients, 41%, 18%, 10%, 4%, and 27% were classified as large-artery atherosclerosis, lacunae, cardioembolism, other determined etiology and undetermined etiology respectively. The most notable difference of this registry from western registries was the predominance of intracranial rather than extracranial location of the large artery atherosclerosis. Hypertension, diabetes and smoking were the common risk factors among all the subtypes. Coronary artery disease and rheumatic heart disease were responsible for most of the cardioembolic strokes. Key words : Stroke subtypes, India, Intracranial atherosclerosis. Introduction Unlike myocardial infarction, acute cerebral infarction (CI ) has various subtypes. These include stroke due to large artery atherosclerosis, disease of small penetrating arteries (lacunae), cardiogenic embolism, coagulopathy, and many nonatherosclerotic vasculopathies.1-3 Many studies have shown that there are significant racial-ethnic differences in the topographical distribution of atherosclerotic lesions.4-12 For example Chinese,4-7 Japanese,8,9 Hispanics, and Blacks,10,11 have a greater preponderance of intracranial atherosclerosis than whites. There is not much data on the stroke subtypes and their risk factors from India. A well organized stroke registry can provide much information and insight into these problems.13-15 The present study was aimed to investigate the frequency and spectrum of various stroke subtypes in a south Indian referral center and to determine if there is any difference in the risk factor profile of various subtypes. Material and Methods The study material consisted of 392 consecutive patients of ischemic stroke enrolled in the Stroke Data Bank (SDB) of Nizam's Institute of Medical Sciences, (NIMS) Hyderabad, between Ist February 2000 to 31st January, 2001. NIMS is a major neurological centre and a University Hospital in Hyderabad, the capital city of south Indian state of Andhra Pradesh. Patients are generally referred by practicing physicians or can get registered themselves. The patient population is fairly representative of the disease pattern in this region. Stroke Data Bank of NIMS is an ongoing, prospective observational project aimed at consecutively collecting the clinical, imageological, laboratory and outcome data on all fully investigated cases of acute stroke. Each patient with acute stroke was examined by a Senior Resident in Neurology, specifically trained in stroke subtype diagnosis, and the findings confirmed by a qualified stroke neurologist within a week of onset of stroke. Information was collected on each patient concerning details of risk factors, past history, general and neurological examination. Patients was investigated according to a fixed protocol, with the aim of delineating the causal mechanism and identifying the risk factors on the pattern practiced in the standard Stroke Data Banks in USA , Europe and South-east Asia.3,15,16 Thus, all patients were required to have a basic minimum of CT scan of brain, extra cranial carotid duplex examination and a 2DEchocardiography. If the stroke mechanism was still not clear, then the patients, depending on the clinical suspicion, were subjected to one or more of additional investigations which included, magnetic resonance angiography (MRA), transesophageal echocardiography, transcranial color-coded duplex (TCCD) study and hematological investigations like collagen profile, estimation of serum homocysteine, and protein C, S and antithrombin III deficiency. However, one or more of these investigations could not be carried out, in the following circumstances : if the patients were too sick to be carried to the particular laboratory, expired before the investigation could be carried out, or the diagnosis was so obvious that no further investigations were necessary. Thus, of all the 392 patients of CI, all underwent CT scan examination of brain, 322 received extracranial duplex examination (82% performance rate), 321 patients received 2D-Echocardiography (82% performance rate), and 252 received intracranial magnetic resonance angiography (64% performance rate). CT scanning was performed on SOMATOM PLUS 4 SIEMENS scanner. MRA was done on 1.5 Tesla GE Sigma Magnetic Resonance Imaging. 3D TOF images were taken at 1.2-1.6 mm thickness slices using 64 location / slab, mostly within 5th to 7th day after the onset of stroke. Colour duplex imaging of carotid arteries was performed on HDI 3000 (ATL) Ultramark 9 unit with linear probe (5-10 MHz) technique. Carotid arteries were examined with the patient's head to the contralateral side. B-mode images were initially obtained in longitudinal and transverse planes to evaluate the plaque location, thickness, extent, morphology (surface and internal appearance), and severity of luminal narrowing of residual lumen. Colour duplex evaluation of stenosis was performed after the B-mode assessment of the carotid arteries. Transcranial colour doppler was performed on the same machine using a dedicated TCD transducer (Sector phased array transducer 2-3 MHz) through transtemporal window. At the time of discharge the stroke patients were subtyped according to TOAST criteria, taking into account all the available data.17 This classification characterizes each stroke by its causal mechanism and takes into account the neurological and medical history, neurological signs, head CT scan, findings from carotid and transcranial duplex sonography, magnetic resonance angiography, electrocardiography and echocardiography. Ischemic strokes were classified into following categories: 1) large-artery disease, either intracranial or extracranial 2) small artery disease (lacune) 3) cardioembolism 4) stroke of other determined etiology and 5) stroke of undetermined etiology. Extracranial Large Artery Atherosclerosis Intracranial Large artery Atherosclerosis Small-Artery Occlusion (Lacune) Cardioembolic Infarction Stroke of other determined etiology Stroke of Undetermined etiology Statistical Analysis The chi square test was employed to find the statistical difference in risk factors between various stroke subtypes. Results Of the 392 patients with CI, there were 282 men and 110 women (mean age 54 years; range 2-97 years). Eighty-eight patients (22%) were younger than 45 years. The frequency, characteristics and prevalence of the stroke risk factors in different subtypes of CI are listed in Table I. No significant difference in age at onset among subtypes of CI was noted except that patients with stroke of other determined etiology were younger than those in other subtypes. Of all the patients with CI, 160 patients (41%) had large artery atherosclerosis (133 intracranial and 27 extracranial). Next in frequency was lacunar infarction in 69 patients (18%). There were 41 patients (10%) with cardioembolic infarcts, the underlying sources of emboli being rheumatic valvular disease in 12, prosthetic valves in 3, wall motion abnormalities secondary to myocardial infarction in 11, intramural clot in 7, complex aortic arch atheromas in 5, atrial fibrillation in 3, and tetrology of Fallot in 1 patient. Stroke of other determined etiology was identified in 17 patients (4%), which included hyperhomocysteinemia in 8, anticardiolipin antibody in 4, Takayasu syndrome in 1, carotid dissection in 2, moya-moya disease in 1 and Protein S deficiency in 1 patient. Despite many investigations, 105 patients (27%) were without an identified cause for their stroke. There was no significant difference in the frequency of risk factors between small and large artery atherosclerosis. However, hypertension was more frequently detected in patients with lacunar infarction than in other stroke subtypes. Within the category of large-artery atherosclerosis, there was no difference in the prevalence of risk factors between intracranial or extracranial atherosclerosis. About one fifth of patients had recurrence in the categories of large artery atherosclerosis, lacunes and cardioembolic strokes. Recurrence was only 12% in the stroke of undetermined etiology and 6% in strokes of other etiology. The combined in-hospital fatality rates of all CI patients was 8.6%. In about 62% of these, the underlying cause could not be identified, as the patients were either too sick to be transported to the laboratories or they expired before the complete investigations could be carried out. However, most of these unclassified strokes had stem blocks with massive hemispherical infarctions, with previous histories of myocardial infarction and therefore presumably cardioembolic nature. Among the remaining expired patients, intracranial atherosclerosis was found in 18%, documented cardioembolism in 14%, extracranial carotid atherosclerosis in 3% and stroke of other determined etiology in 3%. There was no fatality in lacunar infarction group. Discussion Subtyping the ischemic stroke to identify the underlying mechanism is essential for both clinical practice and research. Therefore, a reliable classification system for acute CI is very important. Several clinical classification systems have been used to categorize the subtypes of CI, but one of the more prevalent classifications having a good inter-observer reliability is the one based on TOAST,17 which was adopted for the present study. Of the identified causes of CI, large artery disease was the most common subtype constituting 41% of all strokes. Most of the western stroke registries have reported a similar proportion of large-artery atherosclerosis, though the relative proportion has ranged from 14% to 66%.3,35,37-39 The reason for such a wide range may be influenced by numerous factors, the most important of which are different study designs and definitions of subtypes in various studies (for example in NINCDS Stroke Data Bank, large artery atherosclerosis is defined as > 70% diameter stenosis in the concerned artery whereas other stroke registries use 50% arterial diameter stenosis as the cut-off point), composition of different racial-ethnic populations in different stroke registries and finally, the varying methods of patient selection. While large artery atherosclerosis comprises mostly the extracranial carotid arteries in western registries, it is the intracranial atherosclerosis that formed most of large artery disease in our registry. The racial variation in the pattern and distribution of cerebrovascular lesions is well established, with extracranial carotid atherosclerosis being common lesion found in whites with ischemic stroke, and intracranial arterial stenosis more commonly seen in patients of African, Hispanic, Japanese and Chinese origin.6,12,21-25 There is not enough information on this subject from India. Two earlier studies from India, one based on conventional angiography and the other on MRA, also reported the high frequency of intracranial lesions,26,27 although both of these studies had a limited sample size. Based on the present series, and on our earlier experience, we found that intrinsic intracranial vascular disease was the most frequent lesion of ischemic stroke in our patients.28,29 Such a high frequency of intracranial vascular disease in China, Africa, Japan and now probably India, makes it numerically perhaps the most frequent and therefore the most important cause of stroke worldwide. Yet little is known about the prevalence, natural history, or treatment of this condition. It appears, that the management of patients with intracranial stenosis may differ from that for patients with extracranial stenosis. In a retrospective study of 151 patients with intracranial stenosis, the Warfarin-Aspirin Symptomatic Intracranial Disease Study Group found a favorable risk/benefit ratio for warfarin compared with aspirin for the prevention of major vascular events.30 Patients whose symptoms persist despite anticoagulation and/or antiplatelet therapy, have been shown to benefit by, intracranial angioplasty, with excellent technical results.31 Although conventional angiography is regarded as the gold standard for investigation of the intracranial arteries, this procedure is invasive and associated with significant morbidity. MRA is a non- invasive technique to demonstrate any areas of stenosis. Some patients find MRA expensive, who should at least be screened by TCCD. We, as many others, have previously found that TCCD is a non-invasive, sensitive and much cheaper method, to study intracranial arterial disease. It provides additional information on the hemodynamics of the cerebral circulation. However, in our experience in upto 16% of patients with stroke (depending on age and sex), there was insufficient ultrasound penetration through the temporal bone and it was impossible to perform transcranial Doppler through the temporal window.29 Embolism, although excluded on clinical grounds , is impossible to exclude with certainty. A partially recanalized embolus resembles a stenosis, angiographically. A normal echocardiogram and Holter monitor, relatively but not absolutely exclude cardiac emboli.32 One can, however, make a reasonably confidant diagnosis of intracranial disease in the presence of irregular stenosis, evidence of similar disease in other arteries and lack of cardiac and carotid sources of embolism. Based on our experience and the literature survey, we suggest that all patients with ischemic stroke should be investigated for intracranial stenosis, as it may present as a lacunar stroke and may also co-exist with significant carotid artery disease. It has been observed that intracranial arterial disease is an independent risk factor for developing stroke in patients of symptomatic stenosis of ICA, and carotid endarterctomy may be taken into consideration in these patients even at a lesser degree of stenosis.33 Extracranial carotid atherosclerosis constituted only 7% of all the ischemic strokes, which like oriental countries, is less than that reported from western countries.34,35 Among the known stroke mechanisms, lacunar infarction constituted the second frequent (18%) subtype in our study. This is similar to the data previously reported by us.36 Most of the western stroke registries have also reported lacunar strokes to comprise from 10% to 24%,37-39 except NINCDS and UCDS SDBs where lacunar strokes constituted 27% of strokes, possibly due to the predominance of non-Caucasian population in those areas.35,39 Our percentage of lacunar infarct was less than that reported from Chinese hospital- based studies, such as People's Republic of China (27%),40 Hong-Kong41 and Taiwan.16 It appears therefore that while lacunar stroke is not as frequent in India as in oriental countries, it is still the second known stroke mechanism in India.We found only 10% of our stroke patients to have cardioembolic sources. In most of the previously reported registries from other countries, approximately 20% of the cases were classified as the cardioembolic (CEI) subtype, with no significant difference in this subtype between different races.3,37-39 The main reason for the relatively lower prevalence of cardioembolic strokes among our patients seems to be due to absence of non-valvular atrial fibrillation (NVAF), the biggest contributor of cardioembolic strokes in other registries. The relative paucity of NVAF in our patients is possibly due to lower mean age of our population.43 Also all patients do not undergo transesophageal echocardiography, thereby missing the cardioembolic sources. Interestingly, myocardial wall motion abnormalities following a myocardial infarction were as important as rheumatic heart diseases as the cardioembolic sources.We have reported similar results previously.42 It seems that the rapid urbanization, changing diets, and stressful lifestyle has exposed the population in developing countries to the same risk factors as in developed countries, while the age old risk factors like rheumatic -valvular-heart diseases continue to exist. In our registry and in other registries conducted by Sacco et al,38 and Yatsu et al,44 29% to 40% of the cases were classified as undetermined causes. However, in the studies by Friday et al,45 and Bogousslavsky et al,3 only 1% and 8% of cases were classified as undetermined cases respectively. Hypertension was the most powerful risk factor across all categories, but was most frequent in patients with lacunar infarct (81%), followed next by large artery atherosclerosis (56%) and in infarcts of undetermined etiology (52%). Others have also found similar results.16,46,47 Within the category of large-artery atherosclerosis, there was no difference in the prevalence of hypertension between intracranial or extracranial atherosclerosis. It was less commonly detected in cardioembolic strokes (37%) and strokes due to other etiology (12%). Diabetes mellitus and smoking, as expected were important risk factors among both large and small arterial strokes. The case fatality rate of all CI patients at 1 week was 8.6% which is little higher than reported from other modern registries but comparable to earlier registries. Our study results showed that there was a significant difference in case fatality rates among subtypes of CI. Patients with undetermined etiology had a higher case-fatality rate than the other CI patients, but most of these patients had history of myocardial infarction and had stem blocks; and were presumably cardioembolic in nature. In contrast, patients with lacunar infarcts had no mortality in our registry. In conclusion, stroke due to intracranial large artery disease was the most frequent ischemic stroke subtype in our registry, followed by lacunar disease, cardioembolism and extracranial large artery disease in that order. There was no difference in risk factors within the various stroke subtypes, except that hypertension was much more common in lacunar strokes. There was also no difference in the risk fractors between extra and intracranial large artery atherosclerosis. The etiology remains unknown in about a third of strokes despite extensive investigations. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02157t1.jpg] |
| |||||||||

{kind=link}