
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 50, Num. s1, 2002, pp. S37-S49
|
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002,
pp. S37-S49
Critical Care Management of Acute Stroke
A.K. Meena, A. Suvarna, S. Kaul
Department of Neurology,
Nizam's Institute of Medical Sciences,
Hyderabad - 500 082, India.
Correspondence to : Dr. A.K. Meena, Department of
Neurology, Nizam's Institute of Medical Sciences, Panjagutta,
Hyderabad - 500 082, India.
Code Number: ni02161
Summary
Treatment of acute stroke in an intensive care unit improves the outcome by reducing the
mortality and morbidity. In addition to the primary neurological condition that affects the
outcome, the secondary complications and associated co-morbid conditions also influence
the outcome. It is essential to monitor and maintain the general physiological conditions in
the neurologically sick patients. Maintenance of a clear airway is important to prevent
hypoxic insult to the brain in stroke patients whose airway is compromised. Mean arterial
blood pressure should be maintained > 110mm of Hg. The choice of antihypertensive
is
labetolol. Drugs causing raised intracranial pressure (ICP) should be generally avoided.
Cardiac arrhythmias should be monitored and treated. Treatment of ICP by osmotic
agents is the usual practice. Hyperventilation is reserved for patients who are coning and
is only a temporizing measure prior to surgery. Hemicraniectomy in malignant middle
cerebral artery territory infarcts reduces the mortality significantly. Insulin therapy may
be required to maintain a normoglycemic state for preserving the functionally impaired
neurons. Infections should be treated by appropriate antibiotics. Care should be taken to
prevent aspiration, and deep vein thrombosis. Intravenous thrombolysis for the eligible
candidates and Aspirin for the rest is the recommended therapy for acute ischemic stroke.
Key words : Acute stroke,
Intensive care, Hypertension, ICP.
Introduction
Intensive treatment of stroke especially in stroke units
or intensive care units (ICU) definitely improves
outcome and lowers mortality after stroke.1 There
are
three main areas in the treatment of acute stroke. i)
Treatment of general physiological conditions that
need to be optimized in the setting of acute stroke. ii)
Prophylactic treatment of potential complications
which may be either neurological or medical. iii)
Specific therapy directed against different aspects of
stroke pathogenesis which include treatment for recanalization
and neuroprotection.
Although most stroke patients can be cared for in a
general neurology ward, it becomes important to
recognize when patients with stroke are in need of
more specialized monitoring. Indications for
admission to intensive care units or stroke unit include
requirement for airway management, hemodynamic
monitoring, treatment for increased intracranial
pressure (ICP), observation for neurological
deterioration and patients receiving thrombolytic
therapy.
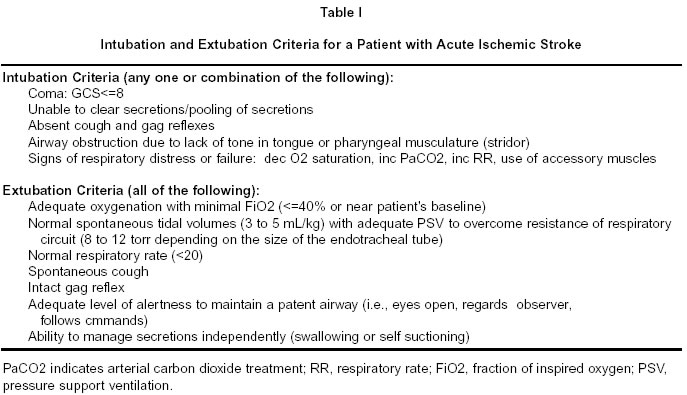
Airway management
Stroke patients may require intubation for either
airway obstruction or acute respiratory failure. Airway
obstruction develops due to three reasons. First, in
acute stroke patients with decreased level of
sensorium the tongue falls backward, intermittently
obstructing the airway, due to lack of tone in the
tongue and pharyngeal muscles. Second, in patients
with brainstem stroke, the gag and cough reflex is
reduced. In addition patients may be unable to clear
the secretions.2 The criteria for intubation
and
extubation are given in table I.3 Stroke patients
may
develop respiratory failure from aspiration or
community acquired pneumonia.
Initial management of intermittent airway include,
placement of oral or nasal airway to prevent
obstruction and allow easier access for suctioning.
Frequent assessments are necessary to check for
sonorous respiration, presence of rhonchi, increased
respiratory rate, decreased oxygen saturation, or
increasing suctioning requirements. Any of these
should alert the physicians to a worsening respiratory
status. Use of mechanical ventilation in a patient with
reduced level of consciousness due to large infarcts
remains controversial. Mortality of 51-90% has been
reported in patients receiving mechanical
ventilation.4-7 These patients are usually intubated
to
secure airway and to institute therapies such as
hyperventilation. Very few patients with ischemic
stroke require intubation (6-8%) and those who do,
have a poor prognosis.7,9 Independent predictors
of
death in patients requiring ventilators include, age,
poor Glasgow coma scale(GCS) score and respiratory
failure.10 Patients with brainstem stroke who
require
ventilator have very poor outcome.10
At the time of intubation, the use of medication, that
provide adequate muscle relaxation, without leading
to haemodynamic instability and prevent elevated ICP
from tracheal stimulation) is recommended.3,11 If
anesthesia is used for intubation, thiopental (3-5
mg/kg IV) can be used in hemodynamically stable
patients whereas, etomide is an ideal drug, in a
hemodynamically unstable patient, but it is short
acting (0.3-0.5m/kg/IV). Propofol (2-2.5mg/kg IV)
can be used but it causes seizures and
hypotension.12,13 Muscle paralysis is usually
avoided,
as frequent neurological examination cannot be
performed. In patients with increased ICP,
neuromuscular blockade should be induced with
vecuronium.14 Succinylcholine is usually avoided
as
it increases ICP and causes hyperkalemia in patients
with neuromuscular disease. Despite all efforts to
avoid hemodynamic compromise during intubation,
hypotension may result especially in aged patients.
Modes of mechanical ventilation : Oral intubation is
the safest method of intubation in patients with
stroke.15 The choice of ventilation is usually
based on
the reasons for intubation, either neurological (airway
protection) or primary respiratory failure. In the
former case, pressure support ventilation is the used.
The amount of additional pressure is adjusted to
achieve a total volume of 5-8ml/kg and a respiratory
rate <25 breaths/minute. Patients with coma or
patients with an abnormal respiratory pattern, need
controlled mechanical ventilation.16 Synchronised
intermittent mandatory ventilation (SIMV) is the
preferred method of ventilation. Positive end
expiratory pressure (PEEP) during ventilation should
be avoided in patients with significantly increased ICP
although setting up to 10cm H2O can be
tolerated.17,18 Patients with impaired oxygenation
(Pneumonia, ARDS, neurogenic pulmonary edema)
require complicated mode of ventilation such as
pressure control, inverse ratio ventilation, high level
of PEEP and inhaled nitrous oxide, If no improvement
is seen within 7-10 days, tracheostomy should be
instituted as early as possible.
Hemodynamic monitoring
Management of haemodynamics in patients with
cerebrovascular disease is complex. Cardiovascular
abnormalities (arrhythmia and blood pressure) are
often responsible for acute neurological illness, such
as stroke and vice versa. Because the risk factors are
shared, patients with cerebrovascular diseases are also
at high risk for cardiac ischemia. Most haemodynamic
manipulation in the neurological intensive care unit
involves : i) management of hypertension in the
setting of an acute neurological insult ii) management
of cardiac arrhythmia and functional cardiac
disturbances concurrent with or caused by acute
neurological insults iii) treatment of vasospasm
following subarachnoid haemorrhage
Management of hypertension : Blood pressure (BP)
management is a critical and controversial issue and
depends on the clinical circumstances.19-24
Hypertension (HTN) is a well-known risk factor for
stroke and 70-80% of patients with acute stroke have
high blood pressure at admission25-27 and BP
spontaneously normalizes over a few hours to 7-10
days.26-28 Continuous BP monitoring should be
done
to avoid the 'white coat effect'.29, 30 In animal
studies
it has been shown that high BP increased the risk of
hemorrhagic transformation. However the data in
human is inconclusive.31-32 Although uncontrolled
HTN might worsen the cerebral edema and outcome
may be poor, experimental data regarding this has
been inconsistent.33 Very few studies in humans
have
shown that treatment of HTN within 24 hours
definitely reduced cerebral edema and improved
outcome in ischemic stroke patients.34 In fact,
review
of the available data in humans has not shown any
convincing link between hypertension at admission
and morbidity and mortality.35-37 Aggressive treatment of BP in
chronically
hypertensive patients might in fact reduce the
cerebral blood flow (CBF) and worsen the ischemic
damage and neurodeficit,37 as cerebral auto regulation
is often set at a higher pressure in chronic
hypertensives , and may actually be impaired in older
people and in patients with ischemic stroke.38-40
Neurons in the penumbral region which are
functionally impaired but still viable, are vulnerable to
the reduction in BP in the face of reduced blood
supply.41 In patients with ischemic stroke who
have
high grade vascular stenosis, lowering of BP might
increase the ischemia and facilitate complete
occlusion of vessels.24 Anecdotal case reports
and
recent studies have shown that lowering of BP was
associated with worse outcome.42,43 SPECT studies
on patients randomized to nicardipine within 72 hours
had shown a decrease in CBF associated with drop in
BP.44
Recommendations for blood pressure management
: As there are no controlled studies addressing the
impact of HTN treatment on outcome in ischemic
stroke, recommendations are largely empirical. The
American Heart Association, suggests that blood
pressure in acute stroke should not be treated unless
patients have severe HTN (mean arterial pressure
>130mm or systolic BP > 220 mm of Hg).45
Occasionally, other serious diseases mandate
aggressive lowering of blood pressure in people with
ischemic stroke. These include acute myocardial
infarction, acute renal failure and dissection of
aorta.23 For patients receiving rt-PA, guidelines
recommend stricter BP control at a systolic pressure
of 185 mmHg and diastolic pressure of 110 mmHg.46
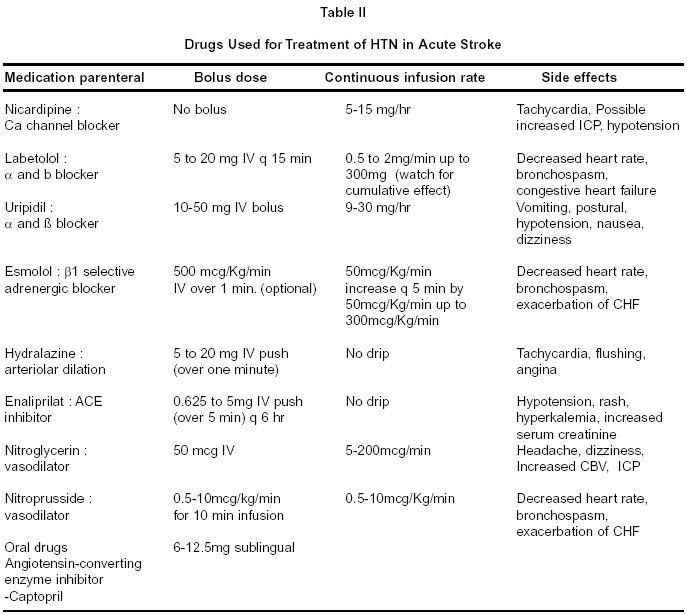
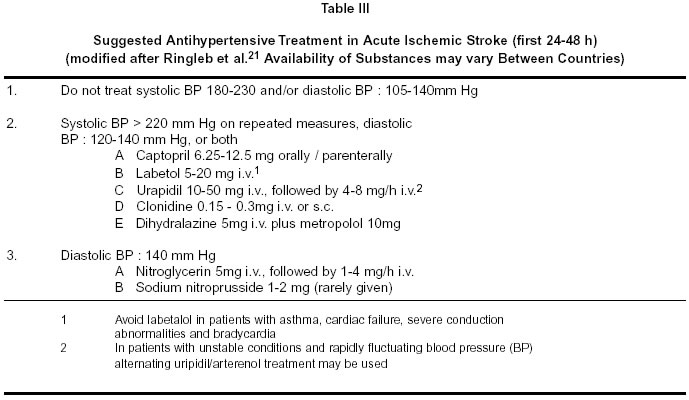
Choice of antihypertensive drug : The most ideal
antihypertensive drug in ICU setting would be the one
with a short half-life, moderate efficacy and devoid
of side effects like sedation. It should not reduce CBF
or ICP. Characteristics of various drugs used in the
treatment of hypertension in acute stroke are
summarized in table II and III. Labetolol, a combined a and b blocker is the ideal drug of
choice.
Angiotensin converting enzyme inhibitors are
preferred because they do not have any effect on ICP
and CBF.47,48 Calcium channel blockers may increase
the ICP but they maintain or increase CBF. When
indicated, we preferably use intravenous labetolol, or
ACE inhibitors in our Intensive Care and Stroke unit.
Conventional drugs, which act as primary vasodilators
such as nitroglycerine, sodium nitroprusside and
hydralazine, can increase ICP and should be used with
caution.
Hemodynamic augmentation
Experimental models of ischemic stroke have shown
that induced hypertension can decrease the infarct size
by increasing the CBF. Studies in humans have shown
that vasopressor use in stroke patients improved the
outcome and it was safer.49,50 However this form
of
therapy needs further evaluation.
ECG changes, cardiac arrhythmias
and myocardial damage
More than 85% of patients with stroke have abnormal
ECGs. New onset ECG changes have been reported
to occur in about 15-30% of ischemic and
hemorrhagic strokes.51,52 These include QT
prolongation, U waves, T wave abnormalities and ST
segment elevation or depression. The exact nature of
these ECG changes is unclear. In many cases the
changes are transient and may be due to stroke itself.
However, many patients have concomitant
cardiovascular disease; 30-65% of patients with stroke
have asymptomatic coronary artery disease.53 In
one
study 15% of patients with stroke were found to have
a coincident myocardial infarction based on ECG
criteria.51 However, accurate data to support
this
incidence of true myocardial damage is scanty.
Elevated CK - MB levels have been found in 11% of
patients, however, these levels rise slowly and peak 4
days after the event unlike true myocardial
infarction.54 These changes are thought to be
due to
increased sympathetic activity and are reported more
frequently with left insular damage.55 There
is one
case report of "stunned myocardium" in stroke similar
to that seen in subarachnoid hemorrhage.56 Stroke
patients have a 25-39% incidence of arrhythmias on
admission ECG, the most common of which is atrial
fibrillation. Holter studies, however, show a higher
incidence of arrhythmias.57,58 Patients with
recent
onset ECG changes have a higher mortality, especially
those with ventricular arrhythmias. Despite this, the
value of routine ambulatory Holter monitoring in
patients with stroke has been questioned because it
does not usually lead to a significant alteration in
management.59
Elevated ICP and brain edema
Ischemic brain edema occurs during the first 24-48
hours after ischemic infarcts. In younger patients with
complete middle cerebral artery (MCA) infarction,
brain edema and elevated ICP may become a major
complication and may lead to herniation and death.60
These patients usually show a rapid decline in
consciousness and develop the signs of herniation 2-4
days after the onset of symptoms. Outcome was fatal
in the majority of these patients, with a mortality of
about 80% with standard treatment.60,61 Appropriate
treatment of raised ICP in large infarcts depends on
the knowledge of ICP and the simplest way is to
measure the ICP by intraparenchymal fiberoptic
pressure monitor. However in patients with large
hemispheric infarcts, the neurologic examination is
more sensitive than the transduced ICP for predicting
outcome.62,63 The insensitivity of ICP monitoring
in
ischemic stroke is most likely related to the fact that
transtentorial herniation occurs because of local tissue
shifts, which are seen before a global rise in ICP.50
General care of patients with raised
ICP
Patient Positioning : Cerebral perfusion pressure
is
optimized when the head of the bed is at 15-30o above
the horizontal.64-66 Because head turning can
impair
jugular venous return, patients should be kept supine
with the head positioned straight ahead.
Intubation : The anesthesiologist should always be
apprised of patients with increased or potentially
increased ICP as this may change their intubation
protocol. For instance, succinylcholine can increase
ICP,67 while standard rapid induction techniques
may
decrease MCA blood 'flow'. In general, induction of
anesthesia should be done with an agent that may have
neuroprotective and ICP lowering effects, such as
midazolam, etomidate or thiopental. The cough reflex,
which can increase ICP, should be suppressed with
lidocaine and neuromuscular blockade achieved with
a non-depolarizing agent like rocuronium or
vecuronium. Aggressive suctioning and neck
procedures should be done with caution.
Fluid management : Raised ICP was historically
managed by fluid restriction in an effort to avoid
increasing brain water. It was later discovered that
hypovolemia could rapidly lead to decrease in
cerebral perfusion pressure (CPP) and thus increasing
the hypoxic-ischaemic injury. Also there is no
evidence that fluid restriction improves brain
edema.67 Free water should be avoided and isotonic
fluids should be given. Normal serum osmolality
should be maintained. Patients should be kept
euvolemic at all times. Hypertension and
hyperthermia should be treated appropriately as both
fever and high BP increase cerebral edema.
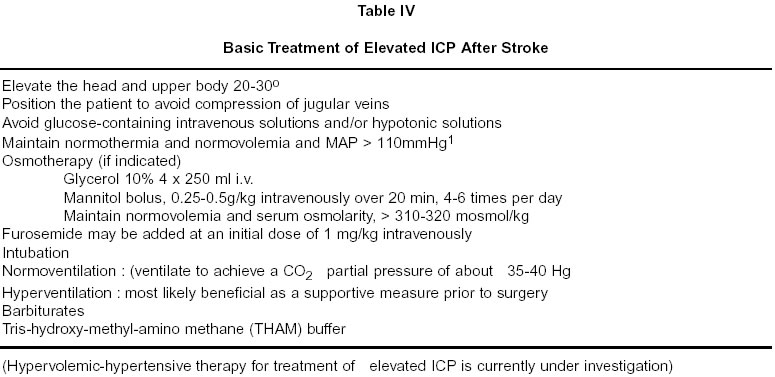
Treatment for increased ICP
Various modes of treatment available for management
of raised ICP are summarized in table IV and are as
follows.
Osmotherapy
Mannitol : Osmotherapy is usually accomplished with
mannitol, which has an osmolality of 5.5 mOsm/kg. In
addition to its osmotic effects, mannitol decreases
blood viscosity and causes vasoconstriction.
Complications of therapy include hypovolemia,
decreased CPP, hyperkalemia, renal failure, and
rebound edema.69 The other osmotic agents are
glycerol and urea, the clinical effects of which are
unproven.
Hypertonic saline
Clinical studies show that hypertonic fluids can
effectively reduce ICP when standard therapies have
failed.70-72 An increase in serum sodium
concentrations to 145 to 155 mmol/L will reduce the
mean ICP and decrease lateral displacement of the
brain in patients with head trauma and postoperative
edema.73 In patients with large hemispheric infarcts,
treatment with hypertonic saline in hetastarch was
found more effective in treating elevated ICP than
mannitol.74 Complications of hypertonic saline
therapy include diabetes insipidus, pulmonary edema,
congestive heart failure, rebound edema and
theoretically, increased mid-line shift.
Hyperventilation
Hyperventilation decreases ICP because it causes
vasoconstriction of the cerebral vessels and thereby
decreases cerebral blood volume (CBV).75 Since
hyperventilation causes vasoconstriction, it can
exacerbate cerebral ischemia.76 Hyperventilation
is
the most effective treatment of acute herniation, but
the efficacy of hyperventilation wanes quickly.77
Chronic hyperventilation also has been associated
with worse outcome in clinical studies.78
Hyperventilation is most effective when CBF is
hyperemic and should be done with SjvO2 (jugular
vein O2 saturation) or AVDO2 (arterio-venous
difference of O2) monitoring.79 Hyperventilation
is
best achieved by increasing the ventilatory rate to 16-
20/sec. The peak effect is achieved within 30 minutes.
Once ICP is stabilized, hyperventilation should be
tapered gradually over 6-12 hours to prevent rebound
increase in ICP.
High dose Barbiturates
Barbiturates are often used to treat patients with
refractory increase in ICP. Barbiturates decrease the
CBF thereby reducing the CBV and ICP.80 Early
experimental studies in stroke suggested that
barbiturates may improve outcome, but a systematic
review of these studies suggest that the benefit was
primarily related to hypothermia.81 In a recent
observational study in patients with large hemispheric
infarcts barbiturate therapy did not improve clinical
outcome.63 Its clinical utility is limited by
systemic
side effects, including hypotension and cardiac
depression, and requires EEG monitoring. Use of
barbiturate coma in stroke is not recommended based
on the existing data.
Induced hypothermia
Small increases in core temperature can lead to
significant increase in CMRO2.83 Induced
hypothermia can be used to treat refractory elevations
in ICP. During hypothermia CMRO2 is reduced there
by decreasing the CBV and ICP.84 Hypothermia
is
found to be neuro-protective in experimental stroke
models. Recently Schwab et al showed that
hypothermia reduces mortality in large hemispheric
strokes. It is also found to be of benefit in head injury
patients.85
Hemodilution
Hemodilution therapy has been popularly used in
stroke treatment especially in European countries.
There are experimental evidences that moderate
isovolemic hemodilution increase CBF and decrease
infarct volume,86,87 but in prospectively randomized
controlled trials hemodilution failed to improve
clinical outcome.88,89
De-compressive surgery
Malignant MCA Infarction : The rationale of
decompressive surgery is to allow expansion of the
edematous tissue away from the lateral ventricle, the
diencephalon and the mesencephalon, to reduce ICP,
to increase perfusion pressure and to preserve CBF by
preventing further compression of the collateral
vessels. These factors may help to increase CBF in
areas surrounding ischemic regions, thereby
preventing further brain tissue necrosis. In large
prospective uncontrolled case series, surgical
decompressive therapy in hemispheric spaceoccupying
infarction lowers mortality from roughly
80% down to 40% without increasing the rate of
severely disabled survivors.61 Early decompressive
surgery (e.g. within the first 24 h after stroke onset)
can reduce mortality even more pronouncedly.90 A
prospective, multicentre study protocol has been
recently developed and is now underway.
Cerebellar Infarction : Decompressive surgery is
widely considered the treatment of choice for a spaceoccupying
cerebellar infarction, although the
scientific basis for this is by no means any more solid
than in hemispheric infarction. Comatose patients
with space-occupying cerebellar infarctions have a
mortality of about 80% if treated conservatively. This
high mortality can be lowered down to 30% if
decompressive surgery is performed.91,92 Like
in
space-occupying supratentorial infarction, the
operation should be performed before signs of
herniation are present. The prognosis among survivors
is very good, even if they were comatose when the
operation was performed. Most of them regain a
Barthel Index of 85 or higher. It should be noted,
however, that these are the results of open, small or
medium-sized case series, one of them prospective,
but mostly retrospective. Data from controlled,
randomized trials are lacking.
Temperature control
Fever is very common in neurointensive care units
(NICU) affecting 30-60% of patients with ischemic
stroke and intracerebral hemorrhage,93 SAH94 and
head injury. Hyperthermia is a proven factor for
cerebral injury in experimental models of focal and
global cerebral ischemia95-97 and its harmful
effect
persists even if it appears days after the start of
ischemia.98,99 The association between hyperthermia,
early neurological deterioration, increased morbidity
and mortality has also been documented in patients
with acute stroke.100 Hyperthermia causes neuronal
injury by several mechanisms.
The cause of post-stroke fever is unclear but in acute
stages it is generally related to the stroke itself, CNS
inflammation or due to the production of endogenous
pyrogens. Fever in the later phases of stroke is usually
due to infectious causes. Although it is generally
accepted that fever should be reduced by aggressive
measures the most effective method remains unclear.
Two types of interventions can be used to reduce
increased body temperature: Antipyretics
(Acetoaminophen, aspirin and NSAIDS) and external
cooling. Antipyretics act by lowering the
hypothalamic set point which is increased in fever.101
Antipyretics are not effective in fever due to an
impaired thermoregulatory mechanism. In such
instances achieving a core temperature of 30oC
requires invasive measures and has potential life
threatening complications. Presently the most
recommended method of external body cooling is aircirculating
blankets, which is minimally invasive.102
Other methods of surface cooling is by ice packs, fans,
water cooled blankets. Fever due to infectious causes
responds to antipyretics combined with aggressive
treatment with appropriate antibiotics.
Glucose metabolism
Both hyperglycemia and hypoglycemia can contribute
to worsening of neuronal injury in acute ischemic
stroke through several mechanisms.103-105
Experimental studies suggest that insulin-induced
normoglycemia may improve stroke outcome.105
Hence monitoring of glucose level in diabetic stroke
patients especially patients on steroids becomes an
important task in intensive care units.106 Aggressive
attempts to normalize blood glucose levels are
recommended especially because combination of
insulin and glucose improves substrate delivery to
ischemic tissue.107 A target blood glucose level
of <200mg/dl is achieved by administering insulin by
sliding scale coverage. If it fails a continuous infusion
may be necessary.
Nutrition
Brain injured patients are hypermetabolic and
hypercatabolic. Therefore, adequate nutritional
support is important for their recovery.108,109 If
a
patient is unable to eat safely, enteral feeding should
be initiated as soon as possible via a nasogastric tube.
Gastric feeding, although the commonest route often,
results in inadequate nutritional support due to
delayed gastric emptying. The ideal enteral formula
should contain adequate caloric intake (25 to 30
Kcal/Kg/day) and avoid hypo-osmolarity and
hyperglycemia.109 To prevent reflux and aspiration
during tube feeding, elevating the head of the bed,
monitoring gastric residuals and administering
metoclopramide (10mg per tube every 6 hours) are
usually effective. Some patients with persistent
delayed gastric emptying will need feedings into the
small bowel. Jejunal feeding is well tolerated and it
enables early, within 72 hours, a high caloric intake
and better nitrogen balance while preventing
regurgitation and aspiration.110 Tube feedings
along
with sucralfate or histamine-2 blockers are used to
prevent stress ulcers.111,112 Care must be taken
to
avoid giving sucralfate at the same time as phenytoin
because it will interfere with phenytoin absorption.
Sedation
Agitation is common in acute stroke.113 Oxygen
consumption is increased in such patients. Short
acting or easily reversible analgesic and anxiolytic
should be used so that clinical examination can be
performed. Propofol is the preferred drug of
choice.114 However short acting benzodiazepins
like
midazolam can also be used.115 These drugs do
not
affect ICP, CPP, and CMRO2. Propofol actually
reduces ICP and CMRO2.116
Deep venous thrombosis (DVT) prophylaxis
An autopsy series of 101 patients with neurologic
disorders found a 24.8% incidence of pulmonary
embolism (PE).117 Stroke patients are at high
risk for
DVT and subsequent PE due to their immobility and
advanced age. Pneumatic compression boots decrease
the incidence of DVTs but not PE in neurosurgical
patients,118 and should be used on all patients
until
they are mobile. The combination of pneumatic
compression boots and low-dose heparin may
decrease the incidence of PE.119 Therefore, patients
at low risk of hemorrhagic complications, such as
those with ischemic stroke, should also be
administered low dose heparin (5000u SC bid).
Neurologic contraindications for subcutaneous
heparin include intracranial hemorrhage (relative),
unprotected intracerebral aneurysm and
hematomyelia.117
Fluid and electrolyte management
Stroke patients should have a balanced fluid and
electrolyte status to avoid plasma volume contraction,
raised hematocrit and impairment of blood rheology
(sludging). Uncontrolled volume replacement leads to
pulmonary edema, cardiac failure and cerebral edema.
In such instances a central venous catheter is
mandatory. Serious electrolyte abnormalities are rare
in stroke. Hyponatremia may occur due to SIADH
(Syndrome of inappropriate secretion of anti diuretic
harmone) or due to excess release of atrial natriuretic
factor (ANF).120 Cerebral salt wasting (CSW)
syndrome is due to centrally mediated renal sodium
wasting.121,122 Existence of CSW syndrome remains
controversial.123 The relation between hyponatremia,
natriuresis and volume depletion is emphasized by
many studies.121,124 SIADH is managed by fluid
restriction or hypertonic saline, whereas
normovolemia should be maintained along with oral
salt supplementation if excess ANF is suspected.
Nosocomial infections
There are very few studies on the prevalence and
incidence of nosocomial infections in neurointensive
care units. The reported incidence varies.125 Review
of the available literature from India shows an
incidence of 18-39 %.126,127 Stroke patients
are at
high risk for silent aspiration, with pneumonia
contributing to 34% of stroke deaths.128 Careful
evaluation of cough and gag reflexes and a thorough
swallowing is essential. Antibiotics are only
recommended if the patient develops signs and
symptoms of infection.129 Intubated patients
have 7-
21 fold higher rate of pneumonia.130,131 The
common
organisms are staphylococcus, pseudomonas,
enterobacter and klebsiella. Initial antibiotics
recommended are a combination of third generation
cephalosporins and aminoglycoside. Urinary tract
infections are the commonest nosocomial infections
with a reported incidence of 30-40%.132 Indwelling
catheter increases the risk by 4-7 times.133
Commonest organisms are gram-negative aerobic
bacilli and they are usually polymicrobial, followed
by the fungi. Blood stream infections are also
common in ICU set up. They are often due to
coagulase negative staphylococcus followed by gramnegative
organisms and candida. Nosocomial
septicemia increases the risk of fatality by 25-50%.134
Empirical treatment should include
vancomycin plus
third generation cephalosporins, pending
the culture
report.
Decubitus ulcers
Frequent
turning
of
immobilized patients
is
useful for
prevention of pressure
sores. The skin of the
incontinent patient must
be kept dry. Air or fluid
filled
mattress system should
be used. If the decubitus
ulcers does not respond
to conservative therapy
antibiotic therapy may
be given for several
days
preceding surgical debridement.
Pharmacotherapy of acute ischemic
stroke
Platelet inhibitors :
The results of two large
randomized, non blinded intervention
studies, namely
International Stroke Trial
(IST) and Chinese Acute
Stroke Trial (CAST)135,136 indicate
that aspirin given
within 24-48 hours after stroke
seems to significantly
reduce mortality and rate of
recurrent stroke. The
positive effect of aspirin may be due to its
effect on
the infarct itself or due to prevention of recurrent
infarction or because of anti inflammatory effect
of
aspirin. Use of heparin, low molecular heparin
or
heparinoids in treatment of acute stroke is not
recommended, because several studies failed to
show
an overall benefit (IST, The TOAST publication
Committee).135,137 Little benefit
even if observed was
counterbalanced by increased number of hemorrhagic
complications. Treatment of stroke in progression
depends on an understanding of the pathophysiology
of the stroke and the mechanism of progression,
whether due to progressive thrombosis or progressing
edema. Anticoagulation is considered the standard
therapy for stroke caused by basilar artery thrombosis
or stenosis and arterial dissections, although
there is
little evidence to support its use in either
situation.
Thrombolytic therapy : Thrombolytic therapy
with
rtPA (0.9 mg/kg body weight) given within 3
hours
after stroke onset is the recommended treatment
of
acute ischemic stroke.46 Intra-arterial
treatment of
acute middle cerebral artery occlusion in a
6-hour
window period using pro-urokinase has also
been
shown to result in significantly improved outcome.138
Conclusion
Most patients with acute stroke do not require ICU
care. It is essential to identify those patients who need
close hemodynamic and airway monitoring. Patients
who are likely to deteriorate and those receiving
thrombolytic therapy should be admitted in ICU. As
the treatment and prognosis in stroke patients are codetermined
by underlying and associated systemic
diseases these problems should be treated with
appropriate medical therapies. Complications, which
arise in ICU, should be identified and treated
accordingly, to ensure better outcome. Thrombolysis
with intravenous rtPA within 3 hours is recommended
for suitable patients of ischemic stroke. In nonthrombolysed
patients, Aspirin administered within
24-48 hours of stroke onset is the recommended
treatment.
References
- Stroke - units Trialists Collaboration : Systematic review
of
the randomized trials of organized inpatient (Stroke Unit)
Care after stroke BMJ 1997; 314 : 1151-1159.
- Borel CO, Guy J : Ventilatory management in critical
neurologic illness. Neurol Clin 1995; 13 :
627-644.
- Deibert E, Diringer MN : The intensive care management
of
acute ischemic stroke. The Neurologist 1999; 5 :
313-325.
- Mayer SA, Boden-Albala B, Bernadini GL et al : Intubation
for life threatening stroke : A population based study
(abstract). Neurology 1997; 48 : A367.
- El-Ad B, Bornstein NM, Fuchs P et al : Mechanical
ventilation in stroke patients : Is it worthwhile? Neurology
1996; 47 :
657-659.
- Cruz-Flores A,
Thimpson DW,
Burch CM et al
: Outcome of
patients with ischemic
stroke requiring
mechanical
ventilation (abstract). Neurology 1997; 48 :
A307.
- Ludwigs UG, Bachrendtz S, Wanecek M et al :
Mechanical
ventilation in medical and neurological diseases
: 11 years
of experience. J Intern Med 1991; 229 :
798-802.
- Gotta J, Pasteur W, Khwaja G et al : Elective intubation
for
neurologic deterioration after stroke. Neurology 1995; 45 :
640-644.
- Gujjar AR, Deibert E, Manno EM et al : Mechanical
ventilation for ischemic stroke and intracerebral hemorrhage
: Indications, timing, and outcome. Neurology 1998; 51 :
447-451.
- Steiner T, Mendoza G, De Georgia M et al : Prognosis
of
stroke patients requiring mechanical ventilation in a
neurological critical care unit. Stroke 1997; 28 :
711-715.
- Diringer MN : Intracerebral hematoma: pathophysiology
and
management. Crit Care Med 1993; 21 : 1591-1603.
- Makela JP, Livanainen M, Pieninkeroinen IP et al : Seizures
associated with propofol anesthesia. Epilepsia 1993; 34 :
832-835.
- Surherland MJ, Burt P : Propofol and seizures. Anaesth
Intensive Care 1994; 22 : 733-737.
- Schramm WM, Strasser K, Bartunek A et al : Effects of
rocuronium and vecuronium on intracranial pressure, mean
arterial pressure and heart rate in neurosurgical patients. Br
J Anaesth 1996; 77 : 607-611.
- Shibutani T, Hirota Y, Niwa H et al : Cerebral arterial blood
flow velocity during induction of general anesthesia: Rapid
intravenous induction versus awake intubation. Anesth Prog
1993; 40 : 122-126.
- Marina PL : The ICU book. 2nd ed. Baltimore: Williams and
Wilkens 1998.
- Burchiel KJ, Steege TD, Wyler AR : Intracranial pressure
changes in brain-injured patients requiring positive endexpiratory
pressure ventilation. Neurosurgery 1981; 8 : 443-
449.
- Cooper KR, Boswell PA, Choi SC : Safe use of PEEP in
patients with severe head injury. J Neurosurg 1985; 63 :
552-555.
- Powers W : Acute hypertension after stroke. The scientific
basis for treatment decisions. Neurology 1993; 43 : 61-71.
- Schrader J, Rothemeyer M, Luders S et al : Hypertension
and stroke - rationale behind the ACCESS trial. Basic Res
Cardiol 1998; 93(Suppl 2) : 69-78.
- Ringleb PA, Bertram M, Keller E et al : Hypertension in
patients with cerebrovascular accident. To treat or not to
treat. Nephrol Dial Transplant 1998;13 : 2179-2181.
- Mzimba ZS, Beevers DG, Lip GYH : Antihypertensive
therapy before, during and after stroke. Basic Res Cardiol
1998; 93 (Suppl 2) : 59-62.
- Spence DJ, DelMaestro RF : Hypertension in acute ischemic
strokes. Treat. Arch Neurol 1985; 42 : 1000-1002.
- Yatsu FM, Zivin J : Hypertension in acute ischemic strokes.
Not to treat. Arch Neurol 1985; 42 : 999-1000.
- Britton M, Carlsson A, deFaire U : Blood pressure course in
patents with acute stroke and matched controls. Stroke
1986; 17 : 861-864.
- Wallace JD, Levy LL : Blood pressure after stroke. JAMA
1981; 246 : 2177-2180.
- Morfis L, Schwartz RS, Poulos R et al : Blood pressure
changes in acute cerebral infarction and hemorrhage. Stroke 1997; 28 :
1401-1405.
- Britton M, Carlsson A : Very high blood pressure in acute
stroke. J Intern Med 1990; 228 : 611-615.
- Harper G, Fotherby MD, Panayiotou BJ et al : The changes
in blood pressure after acute stroke: abolishing the 'white
coat effect' with 24-h-ambulatory monitoring. J Intern Med
1994; 235 : 343-346.
- O'Connell JE, Gray CS : Treating hypertension after stroke. BMJ 1994; 3081 :
523-524.
- Okada Y, Yamaguchi T, Minematsu K et al : Hemorrhagic
transformation in cerebral embolism. Stroke 1989; 20 :
598-
603.
- Shields RW JR, Laureno R, Lichman T et al : Anticoagulantrelated
hemorrhage in acute cerebral embolism Stroke
1984; 15 : 426-437.
- Strandgaarad S, Olesen J, Skinhoj E et al : Autoregulation of
brain circulataion in severe arterial hypertension. BMJ 1973; 1 :
507-510.
- Chamorro A, Vila N, Ascaso C et al : Blood pressure and
functional recovery in acute ischemic stroke. Stroke 1998; 29 :
1850-1853.
- Bourestom NC : Predictors of long term recovery in
cerebrovascular disease. Arch Phys Med Rehab 1967; 48 :
415-419.
- Marquarsden J : The natural history of acute
cerebrovascular disease; a retrospective study of 796
patients. Acta Neurol Scand 1969; 45(S38) : 192.
- Carlberg B, Asplund K, Hagg E : The prognostic value of
admission blood pressure in patients with acute stroke. Stroke 1993; 24 :
1372-1375.
- Wollner L, McCarthy ST, Soper NDW et al : Failure of
cerebral autoregulation as a cause of brain dysfunction in
the elderly. BMJ 1979; 1 : 1117-1118.
- Fieschi C, Angnoli A, Battistini N et al : Derangement of
regional cerebral blood flow and of its regulatory
mechanisms in acute cerebrovascular lesions. Neurology
1968; 18 : 1116-1179.
- Meyer JS, Shimazu K, Fukuuchi Y et al : Impaired
neurogenic cerebrovascular control and dysautoregulation
after stroke. Stroke 1973; 4 : 169-186.
- Astrup J, Siesjo B, Symon L : Thresholds in cerebral
ischemia: the ischemic penumbra. Stroke 1981; 12 : 723-
725.
- Wahlgren NG, MacMahon DG, DeKeyser J et al :
Intravenous Nimodipine West European Stroke Trial
(INWEST) of nimodipine in the treatment of acute stroke. Cerebrovasc Dis 1994; 4 :
204-210.
- Squire IB, Lees KR, Pryse-Philips W et al : The effects of
lifarizine in acute cerebral infarction: a pilot safety study. Cerbrovasc Dis 1996; 6 :
156-160.
- Lisk DR, Grotta JC, Lamki LM et al : Should hypertension be
treated after acute stroke? A randomized controlled trial
using single photon emission computed tomography. Arch
Neurol 1993; 50 : 855-862.
- Adams HP JR, Brott TG, Crowell RM et al : Guidelines for
the management of patients with acute ischemic stroke. A
statement for health care professionals from a special
writing group of the Stroke Council, American Heart
Associataion. Stroke 1994; 25 : 1901-1914.
- The National Institute of Neurological Disorders and Stroke
rt-PA Stroke Study Group. Tissue plasminogen activator for
acute ischemic stroke. N Engl J Med 1995; 333 : 1581-
1587.
- Paulson OB, Jarden JO, Goftfredsen J et al : Cerebral blood
flow in patients with congestive heart failure treated with
captopril. Am J Med 1984; 76 : 91-95.
- Walters MR, Bolster A, Dyker AG et al : Effect of perindopril
on cerebral and renal perfusion in stroke patients with
carotid disease. Stroke 2001; 32 : 473-478.
- Wise G, Sutter R, Burkholder J : The treatment of brain
ischemia with vasopressor drugs. Stroke 1972; 3 : 135-140.
- Rordorf, Cramer SC, Efrid JT et al : Pharmacological
elevation of blood pressure in acute stroke. Clinical effects
and safety. Stroke 1997; 28 : 2133-2138.
- Davis TP, Alexander J, Lesch M : Electrocardiographic
changes associated with acute cerebrovascular disease. A
clinical review. Prog Cardiovasc Dis 1993; 36 : 245-260
- Oppenheimer SM, Hachinski V : The cardiac consequences
of stroke. Neurologic Clinics 1992; 10 : 167-177.
- Chin PL, Kaminiski J, Rout M : Myocardial infarction
coincident with cerebrovascular accidents in the elderly. Age Aging 1977; 6 :
29-37.
- Norris JW, Hachinski VC, Myers M et al : Serum Cardiac
enzymes in stroke. Stroke 1979; 10 : 548-533.
- Oppenheimer SM : Neurogenic cardiac effects of
cerebrovascular disease. Current Op Neurol 1994; 7 :
20-24.
- Wang T, Wu C, Lee Y : Myocardial stunning after cerebral
infarction. Int J Cardiology 1997; 58 : 308-311.
- Norris JW, Frogatt GM, Hachinski VC : Cardiac arrhythmias
in acute stroke. Stroke 1978; 4 : 392-396.
- Rem JA, Hachinski VC, Boughner DR et al : Value of cardiac
monitoring and echocardiography in TIA and stroke patients. Stroke 1985; 16 :
950-956.
- Kessler DK, Kessler KM : Is ambulatory electrocardiography
useful in the evaluation of patients with recent stroke? Chest
1995; 107 : 916-918.
- Hacke W, Schwab S, Horn M et al : Malignant middle
cerebral artery territory infarction : Clinical course and
prognostic signs. Arch Neurol 1996; 53 : 309-315.
- Ricke K, Schwab S, Krieger D et al : Decompressive surgery
in space-occupying hemispheric infaraction: Results of an
open, prospective trial. Crit Care Med 1995; 23 : 1576-1587.
- Frank JI : Large hemispheric infarction, deterioration, and
intracranial pressure. Neurology 1995; 45 : 1286-1290.
- Schwab S, Spranger M, Schwarz S et al : Barbiturate coma
in severe hemispheric stroke : Useful or obsolete? Neurology 1997; 48 :
1608-1613.
- Mixensberger J, Baunach S, Amschler J et al : Influence of
body position on tissue-pO2, cerebral perfusion pressure
and intraacranial pressure in patients with acute brain injury. Neurol Res 1997; 19(3)
: 249-253.
- Feldman Z, Kanter MJ, Robertson CS et al : Effect of head
elevation on intracranial pressure, cerebral perfusion
pressure, and cerebral blood flow in head-injured patients. J Neurosurg 1992; 76(2)
: 207-211.
- Durward QJ, Amacher AL, Del Maestro RF et al : Cerebral
and cardiovascular responses to changes in head elevation
in patients with intracranial hypertension. J Neurosurg 1983; 59(6)
: 938-944.
- Minton MD, Grosslight K, Stirt JA et al : Increases in
intracranial pressure from succinylcholine: prevention by
prior nondepolarizing blockade. Anesthesiology 1986; 65(2)
: 165-169.
- Shackford SR : Fluid resuscitation in head injury. J Intensive
Care Med 1990; 5 : 59-68
- Garcia-Sola R, Pulido P, Capilla P : The immediate and
long-term effects of mannitol and glycetol: A comparative
experimental study. Acta Neurochir 1991; 109 : 114-121.
- Hartl R, Ghajar J, Hochleuthner H et al :
Hypertonic/hyperoncotic saline reliably reduces ICP in
several head-injured patients with intracranial hypertension. Acta Neurochir Suppl 1997; 70 :
126-129.
- Horn P, Munch E, Vajkoczy P et al : Hypertonic saline
solution for control of elevated intracranial pressure in
patients with exhausted response to mannitol and
barbiturates. Neurol Rea 1999; 21(8) : 758-764.
- Schatzmann C, Heissler HE, Koning K et al : Treatment of
elevated intracranial pressure by infusions of 10% saline in
severely head injured patients. Acta Neurochir Suppl 1998; 71 :
31-33.
- Qureshi AI, Suarez JI, Bhardwaj A et al : Use of hypertonic
(3%) saline/acetate infusion in the treatment of cerebral
edema: Effect on intracranial pressure and lateral
displacement of the brain. Crit Care Med 1998; 26(3)
: 440-
446.
- Schwarz S, Schwab S, Bertram M et al : Effects of
hypertonic saline hydroxyethyl starch solution and mannitol
in patients with increased intracranial pressure after stroke. Stroke 1998; 29(8)
: 1550-1555.
- Fortune JB, Feustel PJ, deLuna C et al : Cerebral blood flow
and blood volume in response to O2 and CO2 changes in
normal humans. J Trauma 1995; 39(3) : 463-471.
- Schneider GH, Sarrafzadeh AS, Kiening KL et al : Influence
of hyperventilation on brain tissue-PO2, PCO2, and pH in
patients with intracranial hypertension. Acta Neurochir Suppl
1998; 71 : 62-65.
- Muizelaar JP, van der Poel HG, Li ZC et al : Pial arteriolar
vessel diameter and CO2 reactivity during prolonged
hyperventilation in the rabbit. J Neurosurg 1988; 69(6)
:
923-927.
- Muizelaar JP, Marmarou A, Ward JD et al : Adverse effects
of prolonged hyperventilation in patients with severe head
injury: a randomized clinical trial. J Neurosurg 1991; 75(5)
:
731-739.
- Ausina A, Baguena M, Nadal M et al : Cerebral
hemodynamic changes during sustained hypocapnia in
severe head injury: can hyperventilation cause cerebral
ischemia? Acta Neurochir Suppl (Wien) 1998; 71 :
1-4.
- Miyauchi Y, Sakabe T, Maekawa T et al : Responses of
EEG, cerebral oxygen consumption and blood flow to
peripheral nerve stimulation during thiopentone anesthesia
in the dog. Can Anaesth Soc J 1985; 32 :
491-498.
- Bleyaert AL, Nemoto EM, Safar P et al : Thiopental
amelioration of brain damage after global ischemia in
monkeys. Anesthesiology 1978; 49 : 390-398.
- Yatsu FM, Diamong I, Grazxiano C et al : Experimental
brain
ischemia: Protection from irreversible damage with a rapidacting
barbiturate (methohexital). Stroke 1972; 3 :
726-732.
- Nilsson L, Kogure K, Busto R : Effects of hypothermia
and
hyperthermia on brain energy metabolism. Acta
Anaesthesiol Scand 1975; 19(3) : 199-205.
- Rumana CS, Gopinath SP, Uzura M et al : Brain
temperature exceeds systemic temperature in head-injured
patients. Crit Care Med 1998; 26(3) : 562-567.
- Schwab S, Schwarz S, Aschoff A et al : Moderate
hypothermia and brain temperature in patiens with severe
middle cerebral artery infarction. Acta Neurochir Suppl 1998; 71 :
131-134.
- Cole DJ, Drummond JC, Shapiro HM et al : The effect of
hypervolemic hemodilution with and without hypertension on
cerebral blood flow following middle cerebral artery
occlusion in rats anesthetized with isoflurane. Anesthesiology 1989; 71 :
580-585.
- Perez-Trepichio AD, Furlan AJ, Little JR et al : Hydroxyethyl
starch 200/0.5 reduces infaract volume after embolic stroke
in rats. Stroke 1992; 23 : 1782-1790.
- Haemodilution in acute stroke : Results of the Italian
haemodilution trial. Italian Acute Stroke Study group. Lancet 1998; 1 :
318.
- Multicenter trial of hemodilution in acute ischemic stroke.
Results in the total patient population. Scandinavian Stroke
Study Group. Stroke 1987; 18 : 691.
- Schwab S, Steiner T, Aschoff A et al : Early
hemicraniectomy in patients with complete middle cerebral
artery infarction. Stroke 1998; 29(9) : 1888-1893.
- Heros R : Surgical treatment of cerebellar infarction. Stroke
1992; 23 : 937-938.
- Rieke K, Krieger D, Adams HP et al : Therapeutic strategies
in space-occupying cerebellar infarction based on clinical,
neuroradiological and neurophysiological data. Cerebrovasc Dis 1993; 3 :
45-55.
- Georgilis K, Plomaaritoglou A, Dafni U et al : Aetiology of
fever in patients with acute stroke. J Intern Med 1999; 246 :
203-209.
- Schwarz S, Hafner K, Aschoff A et al : Incidence and
prognostic significance of fever following intracerebral
hemorrhage. Neurology 2000; 54 : 354-361.
- Albrecht RF, Wass CT, Lanier WL : Occurrence of
potentially detrimental temperature alterations in
hospitalized patients at risk for brain injury. Mayo Clin Proc
1998; 73 : 629-635.
- Ginsberg MD, Sternau LL, Glubus MY-T et al : Therapeutic
modulation of brain temperature: relevance to ischemic
brain injury. Cerebrovasc Brain Metab Rev 1992; 4 : 189-
225.
- Meden P, Overgaard K, Pedersen H et al :The influence of
body temperature on infarct volume and thrombolytic
therapy in a rat embolic stroke model. Brain Res 1994; 647
: 131-138.
- Kim Y, Busto R, Dietrich WD et al : Delayed postischemic
hyperthermia in awake rats worsens the histopathological
outcome of transient focal cerebral ischemia. Stroke 1996; 27 :
2274-2281.
- Baena RC, Busto R, Dietrich WD et al : Hyperthermia
delayed by 24 hours aggravates neuronal damage in rata
hippocampus following global ischemia. Neurology 1997; 48 :
768-773.
- Reith J, Jorgensen HS, Pedersen PM et al : Body
temperature in acute stroke: relations to stroke severity,
infarct size, mortality, and outcome. Lancet 1996; 347 :
422-425.
- Holtzclaw BJ : The febrile response in critical care: state of
the science. Heart Lung 1992; 21 : 482-501.
- Mayer SA, Commichau C, Scarmeas N et al : Clinical trial of
an air-circulating cooling blanket for fever control in critically
ill neurologic patients. Neurology 2001; 56 : 292-298.
- Sieber FE, Traystman RJ : Special issues : Glucose and the
brain. Crit Care Med 1992; 20 : 104-114.
- Yip PK, He YY, Hsu CY et al : Effect of plasma glucose on
infarct size in focal cerebral ischemia-reperfusion. Neurology 1991; 41 :
899-905.
- Warner DS, Gionet TX, Todd MM et al :Insulin-induced
normoglycemia improves ischemic outcome in
hyperglycemic rats. Stroke 1992; 23 : 1775-1780.
- Wass CT, Lanier WL : Glucose modulation of ischemic brain
injury: Review and clinical recommendataions. Mayo Clin
Proc 1996; 71 : 801-811.
- Lazar HL : Enhanced preservation of acutely ischemic
myocardium and improved clinical outcomes using glucoseinsulin-
potassium (GIK) solutions. Am J Cardiol 1997; 80 :
90A.
- Young B, Ott L, Norton J et al :The metabolic and nutritional
sequela of the non-steroid treated head injury patient. Neurosurgery 1985; 17 :
784-791.
- Gadisseux P, Ward JD, Young HF et al : Nutrition and the
neurosurgical patient. J Neurosurg 1984; 60 : 219-232.
- Graham T, Zadrozny R, Harrington T : The benefits of early
jejunal hyperalimentation in the head injured patient. Neurosurgery 1989; 25 :
729-735.
- Pingleton SK, Hadzima KD : Enteral alimentation and
gastrointestinal bleeding in mechanically ventilated patients. Crit Care Med 1983; 11 :
13-16.
- Cannon LA, Heiselman D, Gardner W et al : Prophylaxis of
upper gastrointestinal bleeding in mechanically ventilated
patients : A randomized study comparing the efficacy of
surcralfate, cimetidine and antacids. Arch Intern Med 1987; 147 :
2101-2106.
- Henon H, Lebert F, Durieu I et al : Confusional state in
stroke : Relataion to preexisting dementia, patient
characteristics and outcome. Stroke 1999; 30 : 773-779.
- Sanchez-Izquierdo-Riera JA, Caballero-Cubedo RE, Perez-
Vela JL et al : Propofol versus midazolam : Safety and
efficacy for sedating the severe trauma patient. Anesth Anag
1998; 86 : 1219-1224.
- Papazian L, Albanese J, Thirion X et al : Effect of bolus
doses of midazolam on intracranial pressure and cerebral
perfusion pressure in patients with severe head injury. Br J
Anaesth 1993; 71 : 267-271.
- Kelly DF, Goodale DB, Williams J et al : Propofol in the
treatment of moderate and severe head injury : A
randomized, prospective double-blinded pilot trial. J Neurosurg 1999; 90 :
1042-1052.
- Hamilton MG, Hull RD, Pineo GF : Venous
thromboembolism in neurosurgery and neurology patients:
A review. Neurosurgery 1994; 34 : 280-296.
- Black PM, Baker MF, Snook CP : Experience with external
pneumatic calf compression in neurology and neurosurgery. Neurosurgery 1986; 18 :
440-444.
- Frim DM, Barker FG, Poletti CE et al : Postoperative low
dose heparin decreases thromboembolic complications in
neurosurgical patients. Neurosurgery 1992; 30 : 830-833.
- Diringer M, Ladenson P, Stern B et al : Plasma atrial
natriuretic factor and subarachnoid hemorrhage. Stroke
1988; 19 : 1119-1124.
- Cort JH : Cerebral salt wasting. Lancet 1954; 1 :
752-754.
- Peter JP, Welt LG, Sims EAH : A salt-wasting syndrome
associated with cerebral disease. Trans Assoc Am
Physicians 1950; 63 : 57-64.
- Diringer MN, Ladenson PW, Borel C et al : Sodium and
volume regulation in a patient with cerebral salat wasting. Arch Neurol 1989; 42 :
928-930.
- Oh MS, Carroll HJ : Disorders of sodium metabolism:
hypernatremia and hyponatremia. Crit Care Med 1992; 20 :
94-103.
- Reigler R, Schmutzhard E, Skladal D et al : Nosokomiale
infekitonen bei neurologischen intensivpatienten. Eine
retrospective klinische und epidemiologische analyse.
Antibiotic Monitor (Austra) 1990; 6 : 93-95.
- Basavakumar DG : Prospective study of post-operative
infections in neurosurgery. Thesis submitted in partial
fulfillment of regulations of M.Ch Degree in Neurosurgery.
Bangalore University. 1989.
- Khanna N, Arunodaya GR, Umamaheshwar Rao GS et al :
Infections in the Neurology / Neurosurgery ICU: A
prospective study. Neurol India 1999; 47 (Suppl. 1) :
53.
- Roth EJ : Medical complications encountered in stroke
rehabilitation. Phys Med Rehab Clin North Am 1991; 2 :
563-578.
- Bartlett JG, Breiman RF, Mandell LA et al : Communityacquired
pneumonia in adults: Guidelines for management.
The Infectious Diseases Society of America. Clin Infect Dis
1998; 26 : 811-838.
- Cravin DE, Steger KA, Barber TW : Preventing nosocomial
pneumonia: State of the art and perspectives for the 1990s. Am J Med 1991; 91 :
44S-53S.
- Craven DE, Steger KA : Nosocomial pneumonia in
mechanically ventilated adult patients: Epidemiology and
prevention in 1996. Semin Respir Infect 1996; 11 : 32-53.
- Stamm WE, Hooten TM : Management of urinary tract
infection in adults. N Engl J Med 1993; 329 : 1328-1334.
- Amin M : Antibacterial prophylaxis in urology: a review. Am
J Med 1992; 92(Suppl 4A) : 114-117.
- Pittet D, Tarara D, Wenzel RP : Nosocomial bloodstream
infection in critically ill patients. JAMA 1994; 271 :
1598-
1601.
- International Stroke Trial Collaborative Group : The
International Stroke Trial (IST): A randomized trial of aspirin,
subcutaneous heparin, both, or neither among 19,435
patients with acute ischaemic stroke. Lancet 1997; 349 :
1569-1581.
- Chinese Acute Stroke Trial (CAST) : Randomised placebocontrolled
of early aspirin use in 20,000 patients with acute
ischaemic stroke. Lancet 1999; 349 : 1641-1649.
- The TOAST Publication Committee: Low molecular weight
heparinoid, ORG 10172 and outcome after acute ischemic
stroke. JAMA 1998; 279 : 1265-1272.
- Furlan A, Higashida R, Wechsler L et al : Intra-arterial
prourokinase for acute ischemic stroke. The PROACT II
study: a randomized controlled trial. Prolyse in Acute
Cerebral Thromboembolism. Jama 1999; 282 : 2003-2011.
Copyright 2002 - Neurology India.
Also available online at http://www.neurologyindia.com
The following images related to this document are available:
Photo images
[ni02161t3.jpg]
[ni02161t4.jpg]
[ni02161t1.jpg]
[ni02161t2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}