|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S66-S69 Decompressive Craniectomy for Stroke : Indications and Results A.K. Reddy, V. Saradhi, M. Panigrahi, T.N. Rao, P.Tripathi, A.K. Meena* Departments of Neurosurgery and Neurology*,
Nizam's Institute of Medical Sciences,
Hyderabad - 500 082, India. Code Number: ni02165 Summary The role of decompressive hemicraniectomy in stroke victims is gaining popularity among neuroscientists as it is found to be beneficial in malignant infarction of middle cerebral artery (MCA) territory which results in massive edema and brain swelling. Recent articles have showed that this procedure not only reduces mortality but also improves the functional outcome. We report our experience of 32 patients, who underwent this procedure. We found a good outcome in patients in whom the procedure was done early and whose pre operative Glasgow coma scale (GCS) score was 8 and above. It offered no benefit in patients whose pre operative GCS was below 5. Key words : Decompressive craniectomy, MCA malignant infarction. Introduction In large hemispheric strokes, development of 'malignant edema' is a well-known phenomenon. This usually begins on day 2 to 3 following the onset of stroke and mortality in these cases with conservative treatment approaches 80%.1 It is estimated that around 15-20% of patients with such infarcts experience this phenomenon. Failure of medical treatment in this condition has lead to search for alternate methods of treatment to counter the increased intracranial pressure. Idea of removal of a segment of cranial vault to relieve intracranial pressure is one of the oldest neurosurgical concepts. Kocher first described decompressive craniectomy in 1901 for the treatment of posttraumatic brain edema, which was refractory to medical therapy.2 In the landmark article in 1905, Harvey Cushing described the technique of cranial decompression by sub temporal approach in traumatic brain injury patients.3 Since 1950s role of decompressive hemicraniectomies in reducing intra cranial pressure has been reported on and off. We report our experience with this procedure in the stroke victims with herniation syndromes. Material and Methods All patients treated with decompressive craniectomy at Nizam`s Institute of Medical Sciences (NIMS), Hyderabad, India, for stroke during Aug 2000- July 2002 were included for this analysis. Stroke was diagnosed by history, clinical examination and confirmed by CT scan and in some cases by MRI of brain. Selection criteria for decompressive craniectomy were deteriorating sensorium to GCS 12 or below along with evidence of mass effect and midline shift on neuroimaging. Surgery was not under-taken in patients with poorly controlled risk factors and whose infarct territory was other than MCA. Patients requiring surgical treatment were operated with a large fronto parieto temporal free bone flap. Craniectomy was extended till the base of middle cranial fossa. Dura was opened with curvilinear incision with radial extensions. Duroplasty was performed with the temporalis fascia in a watertight fashion. Bone flap was placed in the subcutaneous fat pocket in the right iliac region for cranioplasty at a later date. Scalp flap was closed in two layers without suction drain. All patients were transferred to the neurological intensive care unit for the post operative care. Broad-spectrum antibiotics and post operative anti-edema measures with intravenous Mannitol (1-1.5g/kg/D) were continued for 5 days. Patients were followed up regularly on outpatient basis after discharge from hospital. Results During the 2 years of study period, 32 patients underwent decompressive craniectomy. Men:Women ratio was 25:7 and age range was 17-71 years with a mean of 49 years. Duration of symptoms was 1 to 3 days with a mean of 1day. Interval between admission and surgery was 6 to 48 hours with a mean of 12 hours. Cases were divided into two groups: I (pre operative GCS 8-13) and II (GCS 3-7). In the group I, all patients survived except 2, who succumbed to pulmonary edema and renal failure on 3rd and 4th post operative day, respectively. All the survivors of group I achieved the Glasgow outcome score (GOS) of more than 3 at the follow up. In group II, 11 out of 15 patients died. The survivors of group II had GOS score of 2 on follow up. Age was not found to have any adverse relation to the outcome. Combined mortality of both groups was 40% but the mortality of group II alone was 73%. On the other hand mortality rate was drastically reduced to around 10 % in group I, if the decompression was done early. Right-sided pathology seemed to have a better outcome as 8 out of 13 patients with right-sided infarcts were in GCS 15 at the time of discharge. Compared to pure ischemic infarcts haemorrhagic infarct cases had significantly better outcome in terms of functional recovery. Discussion Reduction in mortality : It has been estimated that 15- 20% patients of MCA infarction experience the phenomenon of malignant brain swelling. The mortality in these patients is 80% and remaining 20% patients remain vegetative for the rest of their lives1,4,5 Conventional anti-edema measures are not effective in controlling this phenomenon, besides causing dyselectrolytemia, rebound intracerebral hypertension, fluid overload, hypotension, cardiac depression and paradoxical intracranial pressure elevation (seen in hyperventilation). Studies in several cohorts of patients with large middle cerebral artery infarction have shown that decompressive surgery can reduce mortality to less than 50%. Our observations confirmed this view, as the overall mortality in our series was 40%. Delashaw et al, in their series of 9 patients reported recovery in 4 patients to a functionally independent state (Barthel Index Score>60).6 Kalia and Yonas et al achieved 100% good outcome in their 4 patients who underwent 'Decompressive Craniectomy'.7 Early intervention : All the reported series being small in size, no clear-cut guidelines have been drawn regarding indications and optimal timing of this procedure.7 In a series of 153 consecutive patients of transtentorial herniation secondary to trauma, who underwent aggressive decompressive surgery, the chance of functional recovery was 30% if done early, but was almost zero in patients with bilateral dilated fixed pupils.8 Richard S Polin et al in their series of 35 cases of bifrontal decompressive craniectomy in severe post traumatic brain edema showed that, if surgery is done within 48 hours, the outcome was better compared to traumatic coma data bank (TCDB) controls.9 Support for earlier intervention was also seen in the experimental stroke study by Doerfler et al, who demonstrated that animals operated on within 4 hours after middle cerebral artery stroke had a significantly better outcome than those on treatment within 12,14 or 36 hours. More interestingly, results showed a significant reduction in infarction size compared with controls. The reasons attributed to the decreased infarct size in early decompression group are, increase in cerebral perfusion pressure and optimization of retrograde perfusion of MCA branches via leptomeningeal collaterals. Thus functionally compromised but viable brain may be able to survive. Though rat and human brain volumes differ and results cannot be equated, this study gave tremendous boost to the proponents of early surgery.10 In 1998, S.Schwab et al in their 6 years open prospective, non-controlled trial concluded that with early decompressive craniectomy (8-42 hours), there was reduction in mortality to 16%, reduction of stay in intensive care unit (ICU) to 7.4 days and improvement in Barthel Index Score (BIS) to 68.8, against matched controls of late decompressive craniectomy who had a mortality of 34.4%, ICU stay of 13.3 days and BIS of 62.6. None of their patients with infarct on dominant side treated early had global aphasia at the end of 1 year.11 Predictors of malignant brain swelling : Since early intervention was shown to produce better outcome, it would be very useful to have predictive tools for detecting patients at highest risk for developing the phenomenon of malignant MCA infarction syndrome. Openheim et al12 noted that those patients whose early diffusion weighted images show infarct volume more than 145ml often progress to malignant edema. In their study, best predictor was infarct volume on diffusion weighted image > 145 cm,3 which achieved 100% sensitivity and 94% specificity.12 Prediction was further improved by bivariate models combining volume diffusion weighted image and apparent diffusion coefficient measurements, which reached 100% sensitivity and specificity in their series of 28 patients. None of the clinical symptoms and signs are early predictors of this malignant phenomenon. Early CT predictors proposed are extent of tissue hypodensity and attenuated corticomedullary contrast. Of course these subtle changes are very difficult to quantify in emergency setting. In early CT scan, hypodensity involving more than 50% of middle cerebral artery territory, was found to be a strong predictor of fatal brain swelling.13 In the above series, early nausea and vomiting in the setting of middle cerebral artery infarct correlated with the malignant progression. No other initial clinical symptoms or signs could be shown to correlate with later malignant brain swelling. None of the other CT parameters like hyper dense MCA sign, hypodense middle cerebral artery territory, hypodense basal ganglia, sylvian fissure obscurations, temporal lobe hypodensity and other vascular territory hypodensities, could be shown to have early predictive value for malignant brain swelling of middle cerebral artery infarcts.13 Mori et al felt, that the CT scan showed significantly higher infarction volume in patients with malignant infarction (288 +/- 62cumm) compared to those patients with non-malignant infarction (200 +/- 56 cumm). Discriminate analysis showed that an infarction volume of more than 240cu/mm was predictive of malignant transformation with 76.4 percent accuracy.14 Evaluation of prognostic factors is the important aspect of case selection. Age : Young age in general has been found to have better functional outcome.15,16 However, age in our patients had no adverse relation to the outcome. Two patients aged above 65 had very good functional outcome. One patient even underwent bone flap replacement. Brain and Pitts showed that after transtentorial herniation in head injuries, the outcome was good in majority of young patients compared to elderly.8 According to Guerra et al2 and Polin et al,9 although specific age for achieving better outcome could not be specified, confirmation of better outcomes in young could be achieved. Grossly , with the increasing age Barthel index score was less at the end of 1 year. According to D. Georgiadis et al the survival rate is independent of patient age and aggressive treatment should not be withheld on the basis of age alone if the treatment is targeted at reducing mortality.16 Glasgow coma score : We found an excellent correlation between preoperative Glasgow coma scale and the ultimate outcome. Among the 32 patients studied by us, those with pre operative score of > 8, had 88% survival and achieved the GOS score of more than 3 at the followup. On the other hand, among those with preoperative GCS below 8, the survival was only 27% and the GOS score was 2 on follow up. Koh, et al found that, patients who presented with GCS of 13 or more had better outcome (50% favourable, 50% unfavourable) compared to those with GCS 12 or below (25% favourable, 75% unfavourable).17 Unresolved issues : Surgical treatment for massive dominant hemisphere is controversial. Aggressive surgical decompression for the dominant hemisphere is clearly life saving, but, the implications for preserving life with severe neurological deficits are less clear.14 Optimum size of hemicraniectomy is still under debate ; it is shown that sub optimal bone windows increase the shear stress leading to hemicraniectomy associated hemorrhages leading to poor outcome. Thus creation of bone defect should be atleast 12cm.18 In one of the study they found correlation between reappearance of basal cisterns to that of more basal decompressive craniotomy defect. Thus adequacy of bone flap removal and tailoring needs to be individualized. We also observed that compared to pure ischemic infarcts haemorrhagic infarct cases has significantly better outcome in terms of functional recovery. We must admit that since our study is not a randomized controlled study and does not have a big sample size, no firm conclusions can be drawn. However, based on our limited experience and from the survey of world literature, certain caveats can be drawn regarding the prognostic factors about the outcome of patients having massive or 'malignant' MCA infarction undergoing decompressive craniectomy.
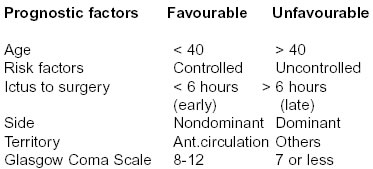
Conclusion Decompressive craniotomy in the setting of acute brain swelling from massive MCA infarct is a life saving procedure. It should be considered in patients with initial good GCS, who are deteriorating in neurological status. With the team effort of neurologist and neurosurgeons these cases have good outcome contrary to the natural history of disease. Preservation of bone flap in the abdominal fat is safe for future placement. Thus an ideal candidate for decompressive craniotomy is the victim who is young, with no risk factors, who presents early and has nondominant, middle cerebral artery territory infarct, with a reasonable Glasgow Coma Scale with no (or) early signs of herniation. The key for success of these cases of large MCA infarcts is early detection. Clinicians should concentrate on formulating newer clinical, radiological and technical protocols to detect the suitable patients at an early stage. Acknowledgements Author is thankful to Smt. Susheela Devi for her secretarial help. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com |
| |||||||||