 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S78-S84 Post Stroke Epilepsy S. Sitajayalakshmi, J. Mani, R. Borgohain, S. Mohandas Department of Neurology,
Nizam's Institute of Medical Sciences,
Hyderabad - 500 082, India.
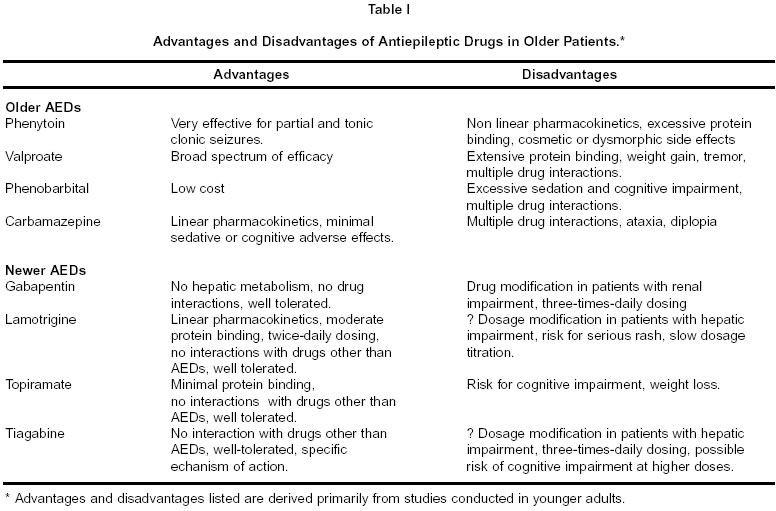
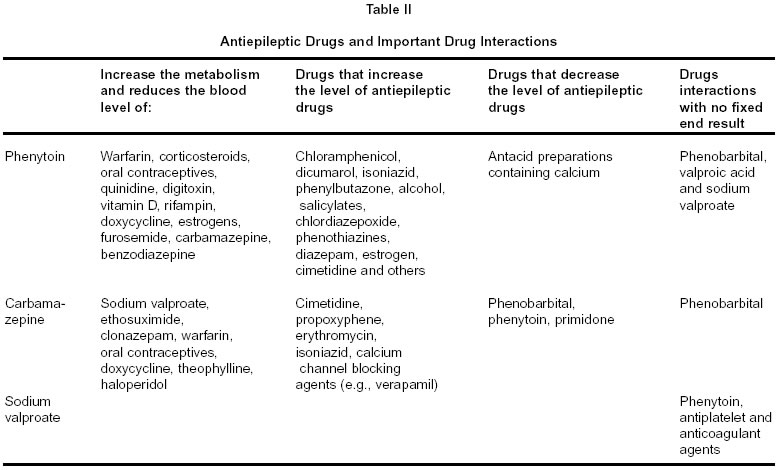
Code Number: ni02167 Summary Stroke is an important cause of acute symptomatic seizures and epilepsy in the elderly. Post stroke early onset seizures occur within two weeks of stroke onset, while late-onset seizures occur after two weeks. The incidence of early seizures is high with lobar hemorrhage, cortical infarcts especially embolic, agitated acute confusional state and increased stroke severity at stroke onset. Both early and late onset post-stroke seizures, left sided cortical infarcts, increased stroke severity and recurrent strokes are the risk factors for post stroke late epilepsy. Post stroke early seizures as well as late epilepsy do not significantly affect long-term outcome and rehabilitation of stroke. Management options for early seizures and late epilepsy vary and need to be individualized. Key words : Stroke, Early seizure, Late epilepsy. Introduction Stroke is one of the most frequent causes of seizures in adulthood, particularly in the elderly. The reported incidence of seizures after stroke varies from 4.1% to 12.5%.1-10 This is related to the different study populations and follow-up times. The incidence of post-stroke epilepsy in India is 13%.11 Despite the relatively low incidence of epilepsy after cerebral stroke, post stroke epilepsy is one of the most common causes of epilepsy due to the high incidence of stroke. Temporal relation of stroke and seizures A seizure may occur before, at the onset of, or weeks to months after a stroke. The incidence of epilepsy prior to stroke was 4.5% when compared to 0.6% in the matched control group.12 This increased incidence of epilepsy in stroke patients may be attributed to sub clinical cerebral vascular disease. These seizures occur weeks or even years before the presenting stroke. Thus the onset of seizures in adult or elderly population may be a warning sign for further strokes and warrants a study of patient's cerebral circulation, especially in the absence of other etiological factors. Post stroke seizures can be classified as early onset seizures, occurring within two weeks following stroke-onset, and late-onset seizures occurring after two weeks. It is important to differentiate between early onset and late onset post stroke seizures as it helps to determine the need and duration to treat these patients with antiepileptic drugs. Post stroke early seizures The combined incidence of epileptic seizures in acute stroke is 4.4% in patients with lobar infarcts, extensive hemorrhages and transient ischemic attacks (TIA).13 The incidence is similar from other studies.14,15 Most of the seizures occur within 24 to 48 hours after stroke.13 Early seizures and stroke type : In a prospective study of 1000 patients with stroke and transient ischemic attacks, the incidence of early seizures was highest (15.4%) in patients with supratentorial lobar or extensive (lobar and deep) hemorrhages, followed by subarachnoid hemorrhage (8.5%), carotid artery cortical infarction (6.5%), and hemispheric TIAs (3.7%).13 Arteriovenous malformation is a common cause of lobar hemorrhage complicated by early seizures. Among the patients with cortical infarcts and early epilepsy, the commonest site of infarction is in the middle cerebral artery territory. Predictably, subcortical and brain stem infarcts, deep cerebral, and infratentorial hemorrhages are not associated with increased risk for seizures. The incidence of seizures is also low (1%) in lacunar infarcts.3 Patients with cerebral embolism experience more seizures than patients with thrombotic infarcts.3,16 Patients with stroke and early seizures had larger lesions on cerebral CT scan (>10mm).13 In the acute stage almost 60% of seizures are partial and the rest are of generalized tonic-clonic type. Of the partial seizures 75% are simple partial motor while the remaining 25% become generalized.13 Predictive factors of early seizures : The presence of precipitating factors like hyperglycemia, hypoglycemia, hypernatremia, hyponatremia, hypocalcaemia, hypomagnesaemia, renal failure and infections - increase the chance of seizures. Atrial fibrillation, and history of diabetes have also been found to be associated with increased risk of early seizures. However the major predictors of early seizures in first-ever stroke patients are cortical involvement in the neuro-imaging studies, agitated acute confusional state at the onset of stroke and initial stroke severity.17,18 Cortical infarcts in carotid distribution were associated with high incidence of early seizures (5% with atheroma in carotid distribution and 20.8% with cardiogenic embolus) in a prospective study of 1,640 patients with first stroke or transient ischemic episode. In addition it was observed that occipital lobe has a high susceptibility for epileptic seizures.3 The area of infarct and surrounding penumbra determine the severity of stroke in the acute state. Single photon emission computerized tomography (SPECT) detects cortical involvement in most patients with early seizures when it is not demonstrated on CT scans. Large lenticulostriate infarcts (>8.3cm3) and ipsilateral cortical (posterofrontal or anterotemporal) ischemic lesions are frequently associated with early seizures.19 Early seizures and prognosis : The functional outcome and mortality of patients with stroke and early seizures are not different from that of stroke patients without seizures.13,18 However, the prognosis during the first few days is worse for patients with seizures than those without; and after the first few days the outcome is similar in both the groups. An early seizure is not a predictor of 30-day case fatality.5 Role of electroencephalography (EEG) : The EEG may show mild nonspecific changes or focal slowing including periodic lateralised epileptiform discharges (PLEDS). Early post stroke seizures- Pathophysiology : Infarct consists of dead tissue in the core surrounded by nonfunctional but potentially viable tissue in the penumbra. In contrast to the dead neurons in the core zone of the infarct, neurons in the penumbra are still alive and able to discharge. Enhanced release of excitotoxic glutamate, ionic imbalances, breakdown of membrane phospholipids and release of free fatty acids in the penumbra play an important role in epileptogenesis. Risk of recurrence : The risk of recurrent seizures in patients with early seizures varies from 11% to 39%.13,20-22 Patients with early seizures are less likely to develop recurrent seizures than patients presenting with late post stroke seizures. Patients with large hemorrhagic strokes, cortical infarcts and lesions involving more than one lobe are at higher risk of developing seizures later.23 Management : There is no data to suggest that prophylactic anticonvulsant therapy is effective against emergence of early seizures. If prophylactic anticonvulsant therapy were to be employed routinely, its use might be limited to the first 24 hours after stroke onset in patients with lobar intracerebral hemorrhage or subarachanoid hemorrhage because almost 90% of seizures occur with in 24 hours of stroke onset.5 Other patients with the highest risk of developing epileptic seizures as per the above mentioned risk factors might also be candidates for prophylactic treatment.23,24 However, there is no data to suggest that prophylactic anticonvulsant therapy prevents seizure recurrence. The indication for treatment in early post-stroke seizures is controversial as the seizures may resolve spontaneously and may not recur. Treatment is indicated only if there is early recurrence of seizures or if the stroke patient presents with status epilepticus. In a retrospective study of AED therapy in patients with early post-ischemic stroke seizures, the seizure free rate after 2 years was 85% in the treated group and 61% in the untreated group. However the subgroup of patients receiving antiepileptic medication immediately after first stroke seizure continue to be at the same rate of risk after treatment was stopped as the untreated group during the first 2 years.25 Seizures can be controlled well with monotherapy.22 Although early seizure occurrence increases risk of subsequent epilepsy, chronic antiepileptic drug (AED) treatment may be warranted only in the presence of cortical involvement caused by infarct or lobar hemorrhage. Status Epilepticus : Early seizures presenting with status epilepticus (SE) were seen in 0.7% to 1.1% of patients with stroke.5,13 Status epilepticus represents 15.8% to 27% of patients with early seizures.5,26 It is common with lobar hemorrhage and subarachnoid hemorrhage than cortical infarcts. Distribution of epileptic types include partial, non-convulsive, generalized and partial with generalized.26 Status epilepticus may occur as a presenting symptom or within the first 14 days after stroke. Although the immediate prognosis of patients with SE is poor, SE as the presenting sign does not necessarily predict subsequent epilepsy. Post-stroke late seizures Although post-stroke late seizures occur after first two weeks of stroke, these may begin months to a year after a stroke. The incidence of post-stroke late seizures is about 15%.27 The interval between stroke and onset of seizures ranges widely. Nearly 24% of seizures occur within 3 weeks and 93% in 2 years. The prevalence of late seizures is high in patients with permanent neurological deficits7 or those needing rehabilitation.27 Primary generalized seizure is common with late onset seizures (56%) compared to early onset seizures, which are generally simple partial in nature. Status epilepticus is more frequent in early-onset than late onset seizures.28 Risk of epilepsy The incidence of recurrent seizures (epilepsy) after stroke in a large prospective multicenter study is 2.5%.2 The possibility of recurrence is greater in lateonset (58%) compared with early-onset seizures (12%).28 In a population based study from Rochester, Minnesota the cumulative probability of developing initial late seizures was 3.0% by 1 year, 4.7% by 2 years, 7.4% by 5 years and 8.9% by 10 years. The risk of recurrence during the first year was 23 times higher for initial late seizures and 17 times higher for epilepsy when compared to population in the community.29 In a retrospective follow up study of 200 consecutive stroke patients 33 developed seizures. Of these 15% developed seizures within the first two weeks after stroke and it increased to 55% by 6 months and at the end of one year all the 33 patients developed seizures.30 Late onset of the first seizure is an independent risk factor for epilepsy after ischemic stroke but not after hemorrhagic stroke.2 However some studies have recorded high prevalence of late seizures in putaminal and lobar hemorrhages.7,9,13 Hemorrhagic infarct, low Rankin scale after the initial seizure and occipital involvement are predictive factors of multiple recurrences.31 Supratentorial brain infarcts, especially cortical is associated with seizure recurrences despite anti-epileptic drug treatment.32 Sub cortical infarcts are associated with infrequent early seizures and a very low one-year risk of recurrence. Patients with a large brain infarct involving the supra-marginal or superior temporal gyrus have 5 times increased risk of late onset seizures, while patients with a cardio-embolic infarct involving the middle temporal or post-central gyrus, had 8 times increased risk of early onset seizures.33 Patients presenting with severe strokes due to total anterior circulation infarction are also at a high risk for recurrent seizures.34 The incidence of late seizures is higher in patients with left cortical infarction (29.3%) than those with right one (15.4%) suggesting that left sided cortical involvement may have some liability to late onset seizures.35 Recurrent stroke increases the risk of initial late seizure or epilepsy.29 Late post-stroke epilepsy - Pathophysiology Late seizures occurring months to years after the stroke are probably due to structural brain abnormalities leading to the development of an epileptic focus when compared to early seizures which result from acute local brain metabolic alteration induced by cerebrovascular event. Early seizures after acute stroke - risk of late seizures : Early seizures are not benign and they constitute an independent risk factor for developing late seizures. Late seizures occurred in 32% of patients with early seizures, compared with 10% of patients whose stroke is not complicated by early seizures.36 Investigations : EEG recordings in patients with late onset seizures may show focal or diffuse slowing or epileptiform discharges, similar to that seen in earlyonset seizures. CT scan may show single or multiple cortical or sub-cortical infarcts. Neurosonography may show carotid occlusive disease. Epileptic seizures are more frequent in patients with carotid stenosis than in carotid occlusion. The neurosonographic findings are similar in patients with early and lateonset seizures and recurrent and non-recurrent seizures.28 Bilateral decrease in the central conduction time along the pyramidal tracts was found in patients with post-stroke epilepsy but not in stroke patients without epilepsy.37 Late onset epilepsy and rehabilitation : Late onset seizures have a minimal impact on rehabilitation and functional outcome.27 On multiple regression analysis, no significant association was found between late onset epilepsy and length of stay, efficiency and effectiveness on Barthel Index and Rivermead Mobility Index, which are the measures of global evaluation of rehabilitation results. Severity of stroke at admission is the most powerful prognostic factor, positively correlating with rehabilitation results and negatively with length of stay. Management : The drug treatment of late onset recurrent seizures is similar to that for patients with epilepsy resulting from other causes. If the patient has previously received AEDs the serum level should be checked and adjusted to more therapeutic levels. In patients with focal motor or generalized seizures as the result of a stroke, carbamazepine and phenytoin have the highest treatment success. Phenobarbital, primidone and valproic acid are second line of choice. Phenytoin is the drug of choice during the acute stage because of the availability of its parenteral form, which can later be switched to the oral form. It has the advantage of once daily regimen but nonlinear kinetics of phenytoin is often a problem. Behavioral changes and sedation are common with phenobarbital. It has been shown in experimental studies that phenytoin, phenobarbital and benzodiazepines impair motor and behavioral recovery after focal brain injury. Among the first line anticonvulsants, carbamazepine offers a linear kinetic profile and is less sedating than phenobarbital. Carbamazepine should be maintained as monotherapy if possible. It may produce hyponatremia and cardiac conduction problems, especially in elderly patients. An acceptable alternative is sodium valproate, which is also well tolerated in elderly and undergoes fewer drug interactions than carbamazepine and phenytoin.38 Sodium valproate and carbamazepine are associated with fewer neuropsychiatric side effects.39,40 This may be important in patients with post stroke epilepsy already having cognitive impairment due to vascular disease. A double blind study supported lamotrigine over carbamazepine in elderly.41 Side effects are common with polytherapy and it should be avoided. Problems with AED therapy : A major determining factor in the treatment of seizure disorders in elderly stroke patients is the side effects of the medications. Dose should take into effect age related changes in pharmacokinetics.42 Age related changes in hepatic and renal physiology alter AED metabolism and elimination. The concomitant drug intake by these patients for behavioral problems, cardiovascular disease, hypertension and infection will alter the distribution and metabolism of AEDs with an impact on efficacy and occurrence of side effects.43 The effect of AEDs on the patient's cognitive function during rehabilitation phase of stroke management is also a limiting factor. The following precautions may help to minimize problems of AED therapy in elderly post stroke epilepsy patients: i) Dose of AED should be carefully selected. Low dose regimens will keep adverse effects to a minimum degree. ii) It should be ensured that the patients are capable of following instructions. If cognitive deficits are significant, family members should be able to take care. iii) Free AED drug levels should be monitored. iv) Patients should be screened for hepatic and renal functions before prescription of AED. Role of newer AED : The first decision confronting the physician is whether to use the conventional AED or one of the newer AED in the elderly patient with post stroke epilepsy. The present knowledge regarding the role of newer AEDs in post stroke epilepsy is limited. Gabapentin may be a good choice due to its safety profile and absence of drug interactions. But its major disadvantages are thrice a day dosing regimen and reduced clearance in renal disease. The advantages of lamotrigine include good overall safety profile, no significant drug interactions and twice daily dosing. It should be considered for patients with severe renal disease because it undergoes hepatic metabolism. The major limiting factor with lamotrigine is the risk of rash. Both topiramate and tiagabine have good side effect profiles and are associated with few drug interactions. At present there is limited data to recommend the use of newer AED in elderly patients. How long to treat : Chronic anticonvulsant therapy is recommended for post stroke late seizures. Patients and their family members should be convinced of the need for long (may be life long) duration of therapy. Most strokes related seizures are partial and partial seizures generally have a poorer prognosis. Presence of neuropsychiatric handicap is another poor prognostic factor, dictating long-term anticonvulsant treatment. Presence of cortical lesions, short periods between seizures, the severity of the seizures and associated toxic metabolic disorders have an adverse effect on the long-term prognosis. Arteriovenous malformations, vasculitis and possible embolic causes of stroke also tend to result in more persistent seizures. The role of EEG in making the decision to discontinue AED is limited. Post stroke late status epilepticus : The incidence of SE in post stroke first time seizure patients is 9% at the end of 3.7 years.46 There is no relationship between the occurrence of SE and stroke risk factors, stroke type, stroke topography, cause, and cortical involvement, size of lesion, and seizure type or EEG findings. SE occurred more frequently among patients with higher disability rating. Early onset SE is associated with a higher risk for SE recurrence. Management is similar to any other SE. Seizures following carotid endarterectomy Seizures are infrequent following carotid endarterectomy (CEA). Seizures may be secondary to cerebral embolisation from the operative site or due to a disturbance of cerebral vascular auto-regulation following CEA leading to a hyper-perfusion syndrome or both. Seizures occur one to two weeks after CEA,47 may be focal or generalized. Lorazepam and phenytoin control the seizures well. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02167t2.jpg] [ni02167t1.jpg] |
| |||||||||

{kind=link}
{kind=link}