 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S94-S101 Botulinum Toxin in Post-Stroke Spasticity R. Borgohain, Bhagyashree,* S Sitajayalakshmi, J. Mani, S. Mohandas Departments of Neurology and Physiotherapy*,
Nizam's Institute of Medical Sciences,
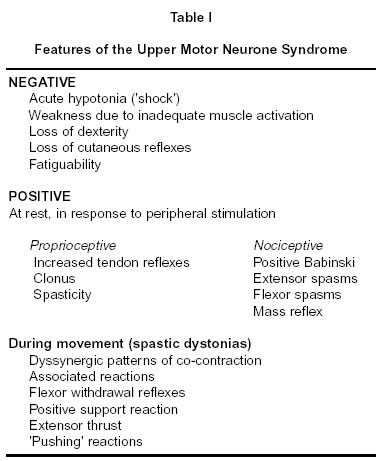
Hyderabad - 500 082, India. Code Number: ni02169 Summary Botulinum toxin therapy is useful in the treatment of post stroke spasticity as seen in many clinical studies. This therapy is always done in conjunction with the physiotherapists. Successful use of botulinum toxin in spasticity requires careful patient and dose selection. Residual function of the spastic limb and the condition of the agonist and antagonist muscles must be carefully assessed. This is to ensure that the overall condition of the patient will improve by inducing partial or complete paralysis of one or more muscles. It is important that the antagonist muscle(s) must have a) sufficiently powerful functional control, or b) be capable of hypertrophy and strengthening if allowed to perform through the appropriate range of motion, or c) be acceptable in the flaccid state. No fixed joint deformity should be present. It is important to check that weakening the spastic limb(s) will not further compromise residual function (including gait). The rationale for the use of botulinum toxin in spasticity is that a velocity-dependant increase in the stretch reflex response in a spastic antagonist muscle may interfere with normal movement in an agonist muscle. However, spasticity may be beneficial in certain situations, eg. leg extension in spasticity may act as a brace in some patients and assist gait. Generally, the side effects associated with botulinum toxin are temporary and well tolerated. The advantages of botulinum toxin are avoidance of anaesthetics, high patient acceptance and persistence of benefit for months. It also facilitates rehabilitation goals, i.e. increased range of motion, ease of hygiene and positioning, and improves quality of life. Its main disadvantage is its high cost. Key words : Botulinum toxin, Spasticity. Introduction Just over a hundred years ago, in 1895, 34 musicians developed a neuroparalytic syndrome after eating raw salted ham in Ellezelles, Belgium. The causative gram positive anaerobic bacterium was isolated and named Bacillus botulinus by Professor E. Van Ermengem; this was subsequently renamed Clostridium botulinum (as per Dasgupta, 1994).1 Van Ermengem established that botulism is caused by the bacterial toxin2 in 1897; Kerner had earlier detailed 230 cases and predicted that the suspected toxin could be eventually used to manage hyperexcitatory states of the central nervous system.3 This, a neurotoxin, is now known as botulinum toxin (BTX),1 one of the most lethal toxins known to the mankind.4 So far 7 antigenically distinguishable serotypes (A,B,C,D,E,F and G) of botulinum neurotoxin produced by seven immunologically different strains bearing the same names, have been recognized.1 Among these, botulinum toxin type A (BTX-A) appears most lethal, only 0.1 microgram of toxin estimated to be capable of causing human death, when taken orally.5 Different serotypes of BTX appear to have different receptors for binding at nerve terminals; these possibly also differ in intracellular site of action, there being at least two different target sites.6 The serotype commercially available for therapeutic purposes is BTX-A. Structure of botulinum neurotoxin The complete aminoacid sequences of BTX serotypes A-F have been deduced on the basis of the corresponding nucleotide sequences. The BTX protein is synthesized as a single chain protein (mol. wt. ~ 150,000), made of 1251 (shortest - the type E) to 1295 (longest - the type A) amino acid residues.1 This protein is cleaved by endogenous proteolytic enzymes leading to the production of dichain BTX protein - consisting of a light (L) chain (mol. wt. ~ 50,000) and a heavy (H) chain (mol. wt. ~ 100,000) linked together by interchain disulfide(s) and noncovalent bonds.1 The proteolytically processed dichain BTX protein is much more (possibly over 100 times) potent than single chain BTX protein and this process of enhancement of biological activity is referred to as activation.7 Study of amino acid sequences of various serotypes of BTX protein reveal an overall low homology (~50%), possibly accounting for antigenic differences. Analysis of secondary structural elements of BTX serotypes A, B and E revealed these proteins to have highly ordered structures. When separated, the secondary structures of the L and H chains do not change significantly, allowing them the capability to express individual biological activities, even when separated.1,7 Site and mechanism of action of botulinum neurotoxin Botulinum toxin acts selectively on peripheral cholinergic nerve endings to inhibit acetylcholine (ACh) release.8,9 Botulinum toxin ordinarily does not cross blood brain barrier and thus does not have significant effect on central nervous system.6 Mechanism of action of botulinum toxin involves following steps : i) Binding : As a first step botulinum toxin binds with high affinity to specific receptors on the presynaptic cholinergic nerve terminal membrane.10,11 The binding is effective even at picomolar concentration or less, accounting for very high potency. Each serotype of botulinum toxin appears to have its own unique receptor,6 the tissue targeting domain of the botulinum toxin molecule being mainly in the H chain.12 Exact nature of toxin specific binding sites is not known. ii) Internalizationion : In the first step, botulinum toxin crosses the plasma membrane by receptormediated endocytosis, becoming entrapped in endosomes. This step is important for action of botulinum toxin as the toxin is susceptible to neutralising antibodies as long as the bound toxin remains on the cell surface. In the second step L chain of the BTX reaches the cytosol. The exact mechanism is unknown but could be a pH-dependant process.13 iii) Intracellular poisoning : L chain of botulinum toxin is responsible for intracellular poisoning.1,6 Experimental data suggest that the toxin is possibly a zinc endopeptidase.14 All serotype inhibit quantal Ach release (serotype A being more potent than others), by rendering the poisoned terminals less sensitive to increased Ca++ levels.6 Botulinum toxin as a therapeutic tool The capacity to produce focal motor denervation with the capability for recovery and almost absent antibody response makes BTX injection an ideal mode of focal neuroparalytic therapy. Side effects of the treatment are usually mild and short lived. However, reinnervation of muscles injected with BTX necessitates repeated injection; this effect of chemodenervation lasts for six to nine months and is dose related. Effect of toxin can be reduced by antitoxin injection into the muscle within 30 minutes of toxin injection. Among the different serotypes of botulinum toxin, BTX-A is the one available commercially. Botulinum toxin injections were first used clinically to correct the imbalance between antagonistic muscles in cases of strabismus.15,16 Since then indications for its use have been continuously growing and most likely will continue to grow in future.17 The greatest impact of BTX-A injection has been in the management of dystonia, as BTX-A injection into the abnormally contracting muscles provides effective relief for most patients with focal dystonia.18 The neurochemical mechanisms underlying dystonia are not well understood. Pharmacological (and surgical) therapy may help some patients, but is usually unsatisfactory in most patients.18 BTX-A injection remains simplest and safest treatment of hemifacial spasm.19 Good results have also been obtained in spasmodic torticollis, writer's cramp, and spasmodic dysphonia. BTX-A injection is now considered the treatment of choice in all forms of focal dystonia (blepharospasm, oromandibular dystonia, spasmodic torticollis, writer's cramp, spasmodic dysphonia, etc.),19 especially so in blepharospasm, spasmodic torticollis, hemifacial spasms and spasmodic dysphonia.17,20 Amongst these, possibly technically the most difficult to inject would be writer's cramp.21 BTX-A injection into the levator palpebrae superior muscle has been used to produce protective ptosis in patients with indolent corneal ulceration or facial nerve damage.22 Some other conditions where it has been found useful are spasticity,23,24 detrusorsphincter dyssynergia in spinal cord injury patients,25 tics26 and tremor. The cholinergic specificity of the toxin, along with the intramuscular route of administration, has proven extremely effective in providing targeted control of muscular activity in various disorders, especially dystonias, as mentioned previously. The use of botulinum toxin type A, from its original indication of treatment of focal dystonias, has rapidly expanded into the treatment of numerous other disorders characterized by excessive or inappropriate muscular contraction.27-29 These include achalasia, anal spasm and vaginismus; eye movement disorders, including nystagmus; other hyperkinetic disorders; and cosmetically troublesome hyperfunctional facial lines (wrinkles). The toxin has also been used to treat other conditions where non-muscular cholinergic chemodenervation may be of benefit, such as hyperhidrosis and sialorrhea.30 Independent analgesic properties also appear to be present in BTX-A, and as such it has been used to relieve the pain associated with conditions in which muscle spasm is a component, eg. back pain and torticollis. This has also been used to treat various forms of headache, especially tension-type headache and migraine. The above list is indicative and not exhaustive. Unwanted effects of Botulinum toxin With repeated injections of BTX-A, therapeutic response in some patients was noted to be abnormally low or even absent. Sera from 28.7% (48 out of 167) of these patients were found to neutralise BTX-A.31 Considering the fact that even subdetectable levels of antitoxin provides significant immunity against BTX, it is possible that rest of patients might have had such levels of antitoxin. The immune response appears dependant upon the total dose of BTX-A received by the patient; the positivity for type A antitoxin ranging from 2.6% of patients receiving 500u or less to 84% of patients receiving 1000u or more.31 Amount of (toxoid) antigen required for active immunisation is usually much more than a patient under treatment would probably receive in a lifetime.31 Hence development of immune response in patients under treatment with BTX-A could be due to one or more of the following: i) higher immunogenicity of toxin (as compared to toxoid), ii) enhancement of immunogenicity by repeated injections of small amounts of antigen, or injection at multiple sites, iii) delivery of more antigen than indicated by the measured biological activity, with biologically inactive toxin molecules acting as toxoid (and contributing to development of circulating antibodies). Theoretically, development of BTX preparations with high-grade purity may allow us to achieve same biological activity with delivery of smaller amount of antigen, in turn reducing the risk of immune response. Immunity, in persons actively immunised against botulism, is long lasting. Hence, it may not be possible to treat effectively patients, with immunity because of BTX treatment, again with the same type of BTX. Other serotypes of BTX once available may prove useful in these patients. Commercially available preparations 'Dysport' and 'Botox' are commercially available in 500u/vial and 100u/vial packs respectively. It is important to note that units of two preparations are not comparable. They also appear to differ in stability, storage conditions etc. Botulinum toxin is commercially available in a frozen lyophilised form. It is very susceptible to damage by mechanical stress, heat and changes in pH. Safety BTX-A is fairly safe if handled correctly. Local side effects are transient. Despite a high percentage of local side effects, patients return for repeat injections. Distant abnormality on single fibre EMG in the form of increased jitter has been reported. However, the clinical significance of this is debated. It is therefore advised to use it with caution in patients with motor neuron disease, myasthenia gravis and myasthenic syndrome. While no absolute contraindications exist, relative ones include pregnancy, lactation and disorders of the neuromuscular junction. Drugs that impair neuromuscular transmission, such as certain antibiotics, anesthetics or other medications also need to be taken into consideration. Role of Botox in post stroke spasticity The annual incidence of stroke in the US is approximately 750,000. Of these roughly a third die, making stroke, after myocardial infarction and cancer, the third leading cause of death. Of the remaining two-thirds, a third are disabled while the remaining recover. Thus many hundreds of thousands of stroke survivors have hemiplegia and impairment of hands and legs. The questions that arise are - what is the contribution of spasticity to this disability and why is BTX-A used to treat it. Spasticity is a complex disorder that causes significant disability in affected patients. There have been numerous definitions of spasticity, which have varied between investigators and publications. A widely accepted definition of spasticity is that it is a motor disorder characterized by a velocity dependent change of muscle tone resulting from a central nervous system insult, categorized by increased resistance of limb to externally imposed motion. While the pathophysiology of spasticity is not completely understood in spite of considerable experimental and human investigation, the increase in tone is generally thought to reflect the loss of descending inhibitory influences resulting in increased excitability of gamma and alpha neurons. In its broader context, one may include spasticity as part of the upper motor neuron syndrome, which includes positive and negative symptoms (Table I). Contralateral hemiplegia or hemiparesis immediately follows injury to the corticospinal tracts. Mild injury, while causing only slight weakness, may cause fatigability and a marked loss of dexterity. These are the 'negative' effects of upper motor neuron lesion while the 'positive' signs include brisk tendon reflexes, Hoffman's and Babinski's signs, dystonia, muscle spasms, clonus and spasticity or increased tone/resistance of muscle to passive movement. The 'positive' signs may appear within days or immediately following the lesion. Thus spasticity may worsen over time causing flexion contractures at the elbows, wrists and fingers and also in the lower limbs.32 These complications are the target of treatment of spasticity. Spasticity impacts not only mobility, but also dexterity, bladder management and bulbar function (Table II). Botulinum toxin is useful in the treatment of spasticity as seen in many clinical studies.33-38 Successful use of botulinum toxin in spasticity requires careful patient and dose selection. Residual function of the spastic limb and the condition of the agonist and antagonist muscles must be carefully assessed. This is to ensure that the overall condition of the patient will improve by inducing partial or complete paralysis of one or more muscles. It is important that the antagonist muscle(s) must have a) sufficiently powerful functional control, or b) be capable of hypertrophy and strengthening if allowed to perform through the appropriate range of motion, or c) be acceptable in the flaccid state. No fixed joint deformity should be present. It is important to check that weakening the spastic limb(s) will not further compromise residual function (including gait). The rationale for the use of botulinum toxin in spasticity is that a velocitydependant increase in the stretch reflex response in a spastic antagonist muscle may interfere with normal movement in an agonist muscle. However, spasticity may be beneficial in certain situations, eg. leg extension in spasticity may act as a brace in some patients and assist gait. EMG guidance, during botulinum toxin injection with teflon coated monopolar needles, while not required for most muscles, can facilitate injection into deeper muscles and in those conditions where it is difficult to identify the hyperactive muscles, such as the lumbricals and other small muscles of the hand. The muscles involved in the common patterns of deformity in the UMN syndrome are listed in Table III.39 As spasticity is a dynamic state and varies depending upon a number of factors such as the initial muscle tone, length of the muscle, and the patient's position, posture and state of relaxation, rating scales help in following the patient response to therapy. These include the modified Ashworth scale,40 Hygiene score, Oswestry scale of grading spasticity (Table IV), global pain scale, global functioning scale, and bilateral adductor scales. However BTX-A treatment needs to be individualised particularly for muscles injected and rigid protocols are inappropriate.41 Both upper33 and lower limb34-38 can be treated with botulinum toxin. In a recently published review, van Kuijk et al42 studied publications from January 1966 to October 2000 on the clinical effects of focal neuronal and neuromuscular blockade in post-stroke upper limb spasticity. They found 10 studies of BTXA of which 4 were randomised controlled trials (RCTs). In addition, they found one uncontrolled observational study on phenol blockade of the subscapular nerve and one on alcohol blockade of the musculocutaneous nerve. These studies were evaluated on 13 methodological criteria. Only 2 RCTs met predetermined criteria of minimal validity. Van Kuijk et al concluded that there was evidence of effectiveness of BTX-A treatment in reducing muscle tone (varying between 0.8 and 2.0 points on the modified Ashworth scale) and improving passive range of motion at all arm-hand levels in chronic stroke patients for approximately 3-4 months. This treatment was deemed to be a safe focal spasmolytic therapy at a critical maximum dose of 100 units of Botox (300-500 units of Dysport) for preserving active finger flexion. The authors further felt that while the effectiveness of BTX-A in improving functional abilities could not be convincingly shown, 2 subgroups who may specifically benefit functionally were - 1) those with mild spasticity and a potential for voluntary extensor activity and 2) those with severe spasticity suffering from problems with positioning and taking care of the affected arm and hand. Brashear et al43 of the Botox Post-Stroke Spasticity Study Group performed a randomised, double-blind, placebo-controlled, multicenter trial to assess the efficacy and safety of one-time injection of BTX-A (200-240 units) in 126 subjects with increased flexor tone in the wrist and fingers after a stroke. The primary outcome measure was a self-reported disability in four areas: personal hygiene, dressing, pain and limb position at six weeks. Each of these was rated on a four-point scale ranging from no disability to severe disability and each subject selected one of these areas in which there was moderate-to-severe disability as the principal target of treatment. The investigators found that there was significantly greater improvement in the BTX-A group compared to the placebo group at weeks 4, 6, 8 and 12 in the principal target of treatment and this difference was statistically highly significant (weeks 4 and 6) to significant (weeks 8 and 12). No major adverse events were reported. This study concluded that disability was reduced in addition to spasticity in post-stroke patients in the upper-limb. The question that remained unanswered in this study was why so many patients had a response to placebo (27%) compared to BTX-A (62%) at week 6. Studies have confirmed the efficacy and safety of BTX-A in lower limb muscles.33,44 Significant positive changes in Ashworth scale44 and on gait analysis variables33 have been found as have been noted in subjective improvement as well. Dose range of Botox varies from muscle to muscle and is more in the lower limb muscles as compared to the upper limb muscles. It varies from 50-240 units per muscle (Dysport 250 - 1500 units) and is injected in 2-6 sites per muscle, with higher doses reserved for larger muscles. In general, the dose should be kept below 300 units per treatment session. Generally, the side effects associated with botulinum toxin are temporary and well tolerated. Most result primarily from diffusion of the toxin into adjacent structures and/or are due to excessive dosages, i.e., weakness in injected and neighbouring muscles. Patients may report subjective symptoms of weakness and fatigue ('flu-like' syndrome) that usually last less than four days. Non-responders are those who fail to exhibit any reduction in muscle tone 4 to 6 weeks after one or more injections. Factors to be considered are a) too low dosages, b) injection technique may require modification, i.e., may require EMG guidance, c) weakness and/or atrophy of injected muscles, with no functional benefit being obtainable, d) a change of pattern in muscle involvement during treatment, e) inappropriate reconstitution or storage of toxin, f) neutralising antibodies as confirmed by in-vivo mouse neutralisation assay. Minimising botulinum toxin dosages and boosters 1-3 weeks later avoid neutralising antibodies. The advantages of botulinum toxin are avoidance of anaesthetics, high patient acceptance and persistence of benefit for months. It also facilitates rehabilitation goals, i.e. increased range of motion, ease of hygiene and positioning, and improves quality of life. Other advantages include effects being local and dose dependent, permitting a selected and graded weakness in injected muscles. If the weakness is excessive, it is temporary. This can also be used in conjunction with systemic medication and the intrathecal baclofen pump. Its main disadvantage is its high cost. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02169t4.jpg] [ni02169t1.jpg] [ni02169t3.jpg] [ni02169t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}