 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, (Suppl. 1), Dec, 2002, pp. S115-S121 Unruptured Intracranial Aneurysms : Review of Natural History and Recommended Management Strategies M. Panigrahi, T. Sanjay, A.K. Reddy Department of Neurosurgery,
Nizam's Institute of Medical Sciences,
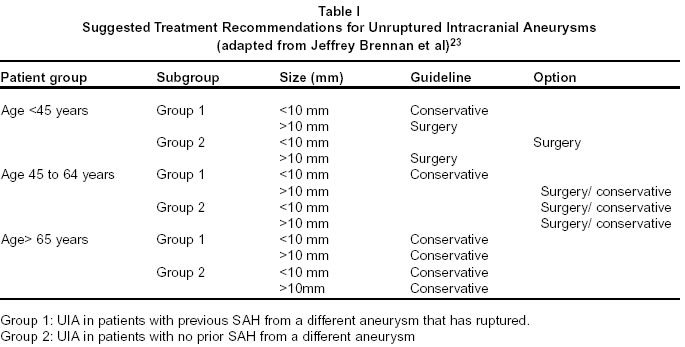
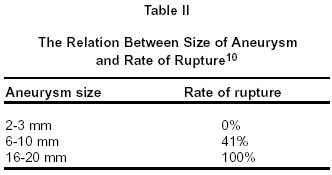
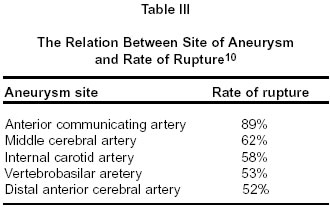
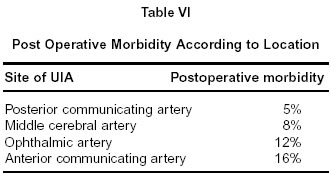
Hyderabad - 500 082, India. Code Number: ni02173 Summary Unruptured intracranial aneurysms (UIA) are common and in the absence of evidence from randomized controlled trials, management decision can be difficult. However with the various well-planned meta-analyses, certain guidelines can be formulated for risk assessment and surgical management. UIA in patients aged more than 64 years irrespective of size, and those measuring less than 10mm in the maximum diameter should be treated conservatively, but should be evaluated yearly with MR angiography or CT angiography to look for rapid increase in size. UIA showing a diameter increase of more than 0.95mm in a year should be treated by surgery or endovascular therapy. Surgery is indicated for all UIA measuring more than 10mm in maximum diameter in patients aged less than 64 years. Endovascular therapy is indicated for UIA, which need intervention but are not surgically accessible or where surgery is contraindicated due to high-risk medical factors. Key words : Subarachnoid hemorrhage, Aneurysm, Unruptured intracranial aneurysms. Introduction Intracranial aneurysms are common,1,2 occurring in an estimated 0.2% to 8.9%3,4 of the general population with a mean frequency of approximately 5%.5,6 Aneurysmal subarachnoid hemorrhage (SAH) carries a high one month mortality rate of about 45%, with approximately half the survivors sustaining irreversible brain damage.7 Approximately up to 15% of stroke cases are secondary to ruptured saccular aneurysms.8 Comparison of prevalence of aneurysms to incidence of aneurysmal SAH (approximately 10 cases per 1,00,000 per year)9 suggests that most aneurysms do not rupture. Unruptured intracranial aneurysms (UIA) refers to the aneurysms with no historical or pathological evidence of a complete breach through the artery walls.10 UIA are classified into symptomatic or asymptomatic, single or multiple and with the presence or absence of previous history of SAH.10 The management of UIA is controversial,11-13 because of a lack of understanding of natural history of these lesions and the risks of repairing them. Although the prevention of hemorrhage has been advocated in recent times as the most effective strategy aimed at lowering mortality rates,14 the optimal management of patients with UIA remains controversial. Management decisions require an accurate assessment of the risks of various treatment options compared with natural history of the condition. The natural history of unruptured intracranial aneurysms and treatment outcomes are influenced by factors such as previous aneurysmal SAH, age of the patient, coexisting medical conditions, aneurysm characteristics such as size, location and morphology and experience of the treating team. There are no prospective randomized trials of treatment interventions versus conservative management to date.8 The studies carried out on UIA have only level IV and level V evidence, which can support grade C recommendations, which present an array of potential clinical actions, any of which could be considered appropriate.15 Natural history Few systematic studies of natural history had been performed before the International Study of Unruptured Intracranial Aneurysms (ISUIA).16 This study enrolled 2621 patients at 53 participating centers in the United States (US), Canada and Europe and had retrospective and prospective components, comprising 1449 and 1172 patients respectively, divided together into group 1 comprising patients with UIA and no history of SAH from a different aneurysm and group 2 comprising patients with UIA with history of SAH from a different aneurysm that has been repaired successfully. It was observed that the risk of rupture of previously UIA less than 10mm in diameter (group 1) was exceedingly low (0.05% per year) compared to that in group 2 (0.5% per year which is 10 times higher). Hence it was concluded in this study that the risk of morbidity and mortality related to surgery greatly exceeded the risk of rupture in group 1 patients with UIA < 10mm and hence need not be clipped. The only predictor of future rupture among these patients was basilar tip location.16 Other studies have found that spontaneous SAH is most frequently caused by aneurysms with a size between 7 to 10mm.17-22 It has been suggested that aneurysm may decrease in size at the time of rupture. Also aneurysms that rupture at the time they form or soon after, may have small critical size. The natural history of UIA was studied by Jeffrey Brennan et al23 by analyzing 45 articles comprising 31,698 patients with 32,292 UIA. Among these there were 14 articles which met the class II evidence, 18 articles contained information on natural history; 19 on risks of surgery and 2 on both, 11 contained analysis of costs and benefits. The suggested treatment recommendations based on conclusions are mentioned in table I.23 Diagnosis of UIA Because UIA are mainly found by serendipity during evaluation of other conditions, the most common types of UIA are those that are part of a multiple aneurysm constellation or those that are symptomatic. The data on asymptomatic UIA is quite small and this accounts for the widespread disagreement concerning how should they be managed. In their review of 3605 UIA, Rinkel et al24 identified that 32% were asymptomatic, 55% were part of a multiple constellation and 13% were symptomatic. In the majority of asymptomatic UIA, current diagnoses are made with the aid of MR imaging and CT scanning which are performed to investigate nonaneurysmal symptoms or events. Current technology is likely to visualize only those UIA which are larger than 3mm in diameter. CT Scan : Standard CT scan with or without contrast agents cannot adequately define the presence or absence of an intracranial aneurysm, particularly if an UIA is suspected.25,26 CT angiography : CT angiography is performed by obtaining images acquired during the arterial phase of contrast opacification. It can demonstrate aneurysms with a size of 2-3mm with sensitivity of 77% to 97% and specificity of 87% to 100%.27 It can be used to follow patients on conservative treatment, those with partially clipped aneurysms, those after endovascular therapy28 and also as a screening tool in populations at high risk for intracranial aneurysms.29,30 Magnetic resonance angiograpy (MRA) : Computer reformation of MRA axial source images helps in displaying several vessels in multiple projections31,32 and can provide additional views which are not possible with conventional angiography. MRA can be used as a good screening modality with a sensitivity of 69% to 93% and is useful particularly, for aneurysms with size ranging from 3-5mm or more.29,33,34 Digital subtraction angiography : This continues to be the gold standard in the diagnosis of intracranial aneurysms. The resolution of images is higher than other forms of angiography,35-37 and it provides information regarding small perforating vessels. This procedure however is not totally safe. Recent studies demonstrate a risk of local catheter related complications of about 5%, permanent neurological morbidity of 0.5% and total morbidity of about 1%. Screening for UIA Noninvasive imaging modalities like CT angiography and MR angiography are fast evolving as the ideal screening modalities for detecting UIA. Important associated diseases with aneurysms are APKD and type VI EDS16,21 and these patients need screening for UIA.38 Familial intracranial aneurysm (FIA) occurs when two relatives, third degree or closer, have radiographically proven intracranial aneurysms. Risk factors for rupture of UIA Aneurysm size : The size dependant aneurysm rupture rates are as per table II. Site of aneurysm : The site dependant aneurysm rupture rates are as per table III. Hypertension : Hypertension was found to be a significant prognostic factor for future SAH whereas surgery reduced the risk of future SAH significantly.10 Rapid increase in the size of aneurysm : This is a significant prognostic factor for rupture and future SAH.42 Treatment Surgery Indications for surgery : Severe progressive related symptoms : Severe progressive symptoms from an aneurysm within the subarachnoid space would be considered by most clinicians to be a good indication for treatment, regardless of the size of unruptured aneurysm. Piepgras39 has stated that symptomatic aneurysm should be subjected to urgent treatment, with the exception of intracavernous ICA aneurysm. In a study of 92 patients who underwent clipping following SAH, 74% of patients experienced headache, eye pain and neck pain. Less frequent symptoms included visual, motor and sensory disturbances.40 In another series, 111 patients with 132 UIA were studied. The presentation was acute in 17%, chronic in 32% and asymptomatic in 51%. The sizes of UIA averaged 2.1, 2.2 and 1.1 mm respectively.41 Increase in aneurysm size : A documented increase in aneurysm size tilts the scales in favour of active treatment, other factors being equal, but some UIA have ruptured without an increase in size. Of 111 UIA followed for almost 19 years in a study by Juvela et al, most were multiple.42 Subsequent rupture of these aneurysms was associated very significantly (p<0.001) with aneurysm growth during the follow-up period. Aneurysms that ruptured had grown significantly than the largest aneurysms harbored in patients who had not experienced rupture (mean growth 6.3mm compared with 0.8mm and 0.95mm per year compared to 0.04mm per year). The mean diameter of aneurysms at the time of rupture was 11.2mm compared with 6mm for the remaining aneurysms, and the mean diameter of fatal ruptured aneurysms was 13.2 mm compared with 10mm for nonfatal ruptured aneurysms.42 Midline site : Sufficient evidence suggests that anterior communicating artery and basilar artery aneurysms should be treated even while they are smaller than laterally situated aneurysms. In 88% of 90 cases in which there were multiple aneurysms, the one with maximum external diameter ruptured.43 When there were multiple aneurysms, the proximal aneurysm ruptured more commonly (70%). However, when anterior communicating artery aneurysm is present, coexisting with proximal aneurysm, the anterior communicating artery aneurysm ruptured more commonly (77%). Anticipated mortality and morbidity rates of rupture : The mortality rate from rupture of previously UIA appears inordinately high and went up to 80%. Among the 49 patients with intact aneurysms, 16% had a rupture at a mean of 4.3 years after diagnosis and out of these, 88% died.44 In the ISUIA, mortality rate was 83% in the group who had no previous SAH compared to 55% in the group who had previous SAH. Aspect ratio : In an effort to find a more reliable basis of differentiation between ruptured and unruptured aneurysms, Ujjie et al45 looked at a ratio which they have called aspect which consists of the ratio of depth of aneurysm to its neck width. They have compared 129 ruptured aneurysms with 78 unruptured aneurysms and observed that no ruptured aneurysm had an aspect ratio of less than 1. In contrast 80% of the ruptured aneurysms had an aspect ratio of more than 1.6. Mortality rate of surgery for UIA A meta-analysis of publications from 1966 to 1992 revealed 28 articles containing data on 733 patients with UIA.52 The mean age was 49 years; male female ratio was 1:1.22, mortality rate was 1% and morbidity rate was 4.1%. In the most exhaustive meta-analysis, Raaymakers et al53 reported a mortality rate of 2.6% in 2460 patients. In 62% of the studies reviewed by them, the mortality was zero. The mortality tended to decrease in the recent years and in accordance with a higher proportion of aneurysms in anterior circulation. Predictive factors for postoperative morbidity of UIA Age more than 64 years : Patients aged more than 64 years had 32% combined morbidity and mortality at 1 year, compared to 14.4% between 45 and 64 years and 6.5% below 45 years (p<0.001).54 Size of aneurysm : The postoperative morbidity of UIA is directly proportional to the size of the aneurysm (Table V).47 Site of aneurysm : The morbidity following surgical clipping of UIA varies according to the location.47 The presence of UIA in the posterior circulation had a higher postoperative morbidity and mortality (Table VI).55 Atherosclerotic or calcified aneurysms : The UIA with these changes had a higher combined mortality and morbidity rate. Among 6 patients with such aneurysms there was a 50% rate of ischemic complications following direct aneurysm clipping.56 Factors independently associated with a high risk of poor outcome or death following clipping of 604 UIA in 493 patients studied prospectively between 1992 and 1999 were patient age (p = 0.05), aneurysm size (p = 0.001), and lesion location along vertebrobasilar circulation (p = 0.08).56 Endovascular treatment Associated morbidity and mortality rates : The mortality rates for endovascular coil embolization have been decreasing over the past decade as technological improvements have occurred. Johnston SC et al have published three studies comparing the results of surgery versus endovascular therapy for UIA.57-59 The first was a cohort study of patients treated at 60 university hospitals between 1994 and 1997.57 Treatment consisted of surgery in 2357 cases and endovascular therapy in 255 cases. Adverse outcome was seen in 18.5% of surgically treated cases and 10.6% of endovascularly treated cases (p = 0.002). The in-hospital mortality rate was higher in surgically treated cases (2.3% compared with 0.4%), but the difference was not statistically significant in the multivariate model. The second series is the one comprising 435 patients treated for UIA at university of California, Sanfrancisco.58 Eighteen patients were operated and 98 were treated by endovascular means. Among the surgically treated group 25% deteriorated by >2 points in the Rankin score, whereas only 8% of endovascular group showed this deterioration. Length of hospital stay was 7.7 days for surgically treated group compared with 5 days for endovascularly treated group. Hospital charges were more for the operated group. At an average of 3.9 years post treatment, 34% of surgically treated patients had persistent or new symptoms compared to 8% in the endovascularly treated group. In the third series, Johnston SC et al mentioned 2699 patients of UIA treated in California between 1990 and 1998.59 Adverse results occurred in 25% of surgically treated group and in 10% of endovascularly treated group. The odds ratio for adverse outcome was 3.1 times greater for surgical group than for endovascular group and that for death was 6.3 times greater for the surgical group. In another study, 120 UIA in 115 patients were subjected to embolisation with GDC coils.60 Complete or near complete occlusion occurred in 91% of aneurysms and incomplete occlusion in 4%, but 5% could not be treated by coiling at all. Clinical deterioration from procedural complications occurred in 4.3% of patients. All these complications occurred in the initial 50 patients, and none in the later 65 patients. One partially embolised aneurysm ruptured 3 years after coil embolization. A systematic review of 48 studies,61 totaling 1383 patients revealed permanent complications in 3.7%, complete occlusion in 54% and more than 90% occlusion in 90% of aneurysms respectively.Weighted linear regression analysis of outcome measures with aneurysm type, clinical condition before embolization, aneurysm size, and aneurysm neck size did not show any statistically significant relation with complications. Compared to patients treated with controlled detachable coils, functional outcome was worse in patients treated with pushable coils, which are now being replaced in clinical use by the former. The post procedure mortality was 7%. Conclusions With the rise in practice of noninvasive neurovascular imaging, UIA are being detected with increasing frequency, posing a management dilemma for the treating physicians. A properly designed prospective randomized control trial would provide appropriate guidelines, but the possibility of such a trial in the near future seems unlikely due to the complexity of design and the risk involved for patients being included in the conservative treatment group. Based on the review of current world literature following guidelines for management of UIA seem justified : i) UIA, irrespective of size, in patients aged more than 64 years should be treated conservatively. ii) UIA measuring less than 10mm in the maximum diameter should be treated conservatively. iii) Patients with UIA undergoing conservative treatment should be evaluated yearly with MR angiography or CT angiography to look for rapid increase in size. iv) UIA on conservative management which show an increase of more than 0.95mm in an year have to be treated by surgery or endovascular therapy. v) Surgery is indicated for all UIA measuring more than 10mm in maximum diameter in patients aged less than 64 years. vi) Endovascular therapy is indicated for UIA which need intervention but are not surgically accessible and in such cases where surgery is contraindicated due to high risk medical factors. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02173t2.jpg] [ni02173t6.jpg] [ni02173t4.jpg] [ni02173t3.jpg] [ni02173t5.jpg] [ni02173t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}