 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
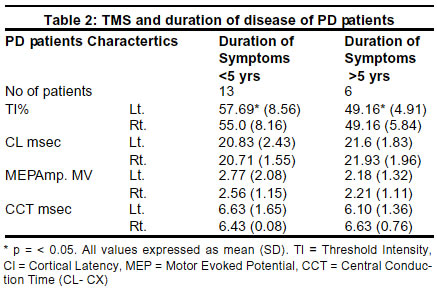
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 13-15 Increased cortical excitability with longer duration of Parkinson's disease as evaluated by transcranial magnetic stimulation M. Bhatia, S. Johri, M. Behari Department of Neurology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029, India. Accepted on 01.03.2001. Code Number: ni03001 Transcranial Magnetic Stimulation (TMS) was used to evaluate the cortical excitability and central motor pathways in Parkinson's disease (PD) and correlate with severity and duration of disease. 19 cases of PD and 13 controls were enrolled. The threshold intensity (TI), cortical latency (CL), central conduction time (CCT), motor evoked potential amplitude (MEP) obtained with TMS were correlated with Hoehn and Yahr and duration of disease. The threshold intensity (TI) was significantly lower in patients of PD than controls. The TI in patients with PD was 53.16+ 8.4% patients and 67.1+21.6% in controls (p<0.05). This strongly correlated with duration of disease, TI being lower in patients with disease duration more than 5 years. There was no difference in the other TMS parameters CL, CCT, MEP between patients and controls.Our study revealed increased excitability in PD which was related to longer duration of disease. Key Words: Parkinson's disease, Cortical excitability, TMS. Transcranial magnetic stimulation (TMS), originally described by Barker et al1 has now evolved into a safe, non-invasive method of stimulating intact motor cortex in humans and thereby enabling assessment of conduction in central motor pathways and excitability of motor cortex.2,3 Several studies have been done to evaluate central motor circuitry in Parkinson's disease in an effort to understand the pathophysiologic mechanism.4,5 Reports of the previous studies of TMS in PD have been very heterogeneous with different parameters being evaluated by authors. The reports include an increase in amplitude of motor evoked potential (MEP) as compared to controls,4,6,7 a decrease in latency on the rigid side,8 decrease in threshold on more affected side, 3,4,9 an increase in threshold10 while others reported changes in central motor conduction time.4 The effect of duration and disease severity on these parameters has however not been adequately studied. The aim of this study was to use TMS to study the motor cortex excitability and central conduction in patients with Parkinson's disease as compared with healthy controls. Material and Methods We studied 19 patients with Parkinson's disease attending the Movement disorders clinic at the All India Institute of Medical Sciences, New Delhi, India between Jan 1997 to June 1998. The clinical diagnosis was as per the criteria by U.K. Parkinson's Disease Society Brain Bank clinical diagnostic criteria.11 All subjects gave written informed consent prior to the study. Patients with poorly controlled tremors at rest, metallic implants such as cardiac pacemaker, intracranial aneurysmal clips, urinary bladder stimulator and metallic orthopedic implants, pregnant women, those with poorly controlled seizures and with severe on-off phenomenon were excluded. Controls included healthy volunteers and relatives of patients admitted in neurology ward. None had a prior history of neurologic disease or metallic implants. Magnetic stimulation of cortex and cervical spine was done with D-190 circular magnetic coil (Digitimer Limited, Hertfordshire, U.K.) 9 cm,1.5 tesla with maximum coil energy of 1200 joules. Cortical stimulation was done with coil positioned tangential to skull, over the vertex in mid-saggital plane, dissecting the intraural line. The direction of current was anticlockwise for stimulation of right cortex and clockwise for stimulation of left cortex. Cervical stimulation was done with center of coil placed over 7th cervical spinal process. Stimuli were delivered as single shocks at least 5-10 seconds apart.12 Standard Medelec EMG machine (Oxford, UK) was used for recording MEP from abductor pollicis bevis (APB) by surface electrodes. Subjects were seated comfortably in a chair, with their arms in their lap and eyes open. Activation of APB was achieved by abduction of thumb to 450 against gravity. The threshold intensity, cortical latency, MEP amplitude and central conduction time on both sides in each patient and control were recorded. Threshold Intensity (TI): This was determined for the relaxed muscle ensured by recovery EMG. TI was defined for each hemisphere, as lowest stimulation intensity required to evoke at least three reproducible MEPs out of five consecutive stimuli at rest with peak to peak amplitude of more than 50 micro volts,12 at a sensitivity of 200 microvolts. Cortex was initially stimulated at 25% of maximum coil output. Intensity was increased in 5% increments with 5 stimuli given at each intensity. If no response was recorded at maximum output of 100%, then thumb was abducted to 450 for activation of target muscle. In the absence of response the TI was taken as 100%.12 Cortical Latency (CL): Cortical latency was determined with activation of target muscle. Five stimuli of 30% above T1 were given. CL was defined as shortest interval between time of stimulation and onset of first negative wave of MEP. Cervical Latency (Cx): It is time taken by electrical stimuli to travel from spinal motor neurons to target muscle i.e. APB. Cx was determined by stimulating afferent roots at the C7 vertebral level. Central Conduction Time (CCT): Statistical analysis was done using analytical software 92, Statistic version 4.0. The mean and SD of TI, CL, MEP amplitude and CCT were compared in Parkinson's disease patients and controls, using t-test with p< 0.05 considered as significant. Intra-group analysis of PD patients was done to correlate the findings with duration of disease, stage of disease (H and Y) and type of Parkinson's disease (`tremor dominant' versus `akinetic rigid type'), predominant side affected using rank-sum two sample (Mann Whitney) test. Results Transcranial magnetic stimulation (TMS) was done in 19 cases of Parkinson's disease and 13 controls. The mean age of PD patients was 56.5+10 years and 41+ 11 years in controls. TI was significantly lower on both sides in PD patients (p < 0.05) as compared to controls. There was no significant difference between patient and control on either side with respect to cortical latency (CL), amplitude of motor evoked potential (MEP amp), central conduction time (CCT) (Table 1). TMS analysis of 11 tremor dominant and 9 akinetic rigid patients revealed no significant difference in the parameters tested (TI, CL, MEP amplitude and CCT) on either side in the two groups. Two subgroups were created signifying severity of disease. One group was with H and Y stage 1 and 1.5 i.e. unilateral disease (n=9): and second group with H and Y>2. The TI, CL, CC and CCT revealed no significant difference. 14 patients out of 19 had predominant left-sided affection and 5 had right-sided affection. There was no significant difference in any of the values on either side. Patients with duration of symptoms less than 5 years (n=13) were compared with patients having duration of symptoms more than 5 years (n=6). TI was significantly less in patients with >5 years duration, signifying increased excitability of motor cortex as the disease advances (Table 2). Discussion In the present study the threshold index (TI) was significantly lower bilaterally in PD patients as compared to controls (P value <0.05). This has also been reported by Cantello et al.6 The other parameters such as cortical latency (CL), motor evoked potential (MEP) amplitude and central conduction time (CCT) did not show a statistical difference when compared to controls. The reports on TMS have heterogeneous findings. Kandler4 has observed a decrease in CCT, however others 6,9,13 have found no change in CCT. The present study also did not find any difference in CCT in patients as compared to controls. Valls-Sole et al8 and Ridding et al5 have reported no difference in TI, but reported an increase in MEP amplitude, decrease in cortical latency (CL) and loss of facilitation with active contraction of muscle in PD patients as compared to controls.8 On the other hand, Davey et al10 and Ellaway et al13 have reported increase in TI on more bradykinetic side in Parkinson's disease. There are only a few studies4,6 evaluating the relationship between disease severity, duration of disease and predominant type of PD (akinetic rigid vs. tremor dominant) with TMS parameters. Both the studies have reported decrease in TI in PD, but found different results of CCT. While Kandler4 reported decrease in CCT in patients with predominant rigidity and bradykinesia, Cantello6 found no significant change in CCT. The present study revealed no difference in any of the TMS parameters, including TI in the two broad clinical categories of `tremor dominant PD' and `akinetic rigid PD'. However, there was a consistent and significant correlation of TI, with disease duration. TI was found to be significantly lower in patients with disease duration more than five years (p<0.05) as compared to patients with disease duration less than five years. This may suggest that excitability increases with increasing duration of disease, however there was no difference on comparing with severity of disease. An increase in MEP amplitude has been reported by some studies.4,6,7 This was not observed in the present study. Various mechanisms have been proposed for the increased amplitude, such as increased facilitation. The pathophysiology of PD rigidity is largely obscure but together with other factors there may be excessive drive to alpha motor neurons (a-MNS) from supraspinal structures. Rubro-, reticulo- or vestibulo- spinal pathways could transmit this uncontrollable drive to a-MNS when released from basal ganglia, where the primitive dysfunction lies. The clinical and electrophysiological significance and implications of these conflicting results are not clear. It appears that the relationship, which may exist between the electrophysiological abnormalities and individual clinical features and severity of disease, may be more complex or an expression of some other aspect of pathophysiology of PD which should be explored further. Acknowledgments The authors acknowledge the technical assistance provided by R.S.Arya and M.S.Bisht and secretarial assistance by Laxmi Rawat. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03001t1.jpg] [ni03001t2.jpg] |
| |||||||||

{kind=link}
{kind=link}