 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
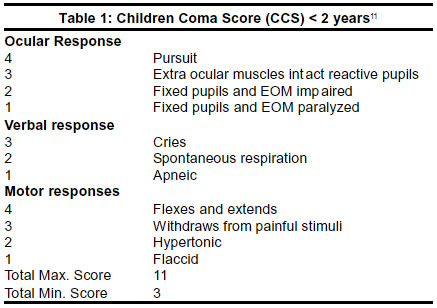
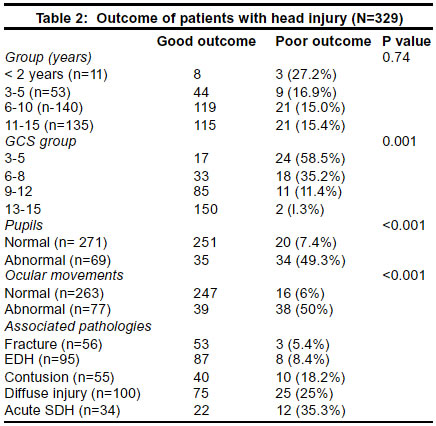
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 16-18 Prognosis in children with head injury: An analysis of 340 patients H. S. Suresh, S. S. Praharaj, B. Indira Devi, D. Shukla, V. R. Sastry Kolluri Department of Neurosurgery, NIMHANS, Bangalore-560029, India. Accepted on 24.07.2001. Code Number: ni03002 Background: The outcome in children with head injury is distinctive because of the different biophysical properties of the child's skull and brain, and their reaction to injury. Methods: In this retrospective study of three hundred and forty children with head injury, managed from January 1993 to December 1998, at NIMHANS, the factors influencing outcome were analyzed. Results: On admission there were 40 children in GCS 3-5, 55 children in GCS 6-8, 96 in GCS 9-12 and 152 children in GCS 13-15. Eleven patients were under 2 years of age, 53 were between 3-5 years, 140 were between 6-10 years and 156 were between 11-15 years of age. The prognosis in various intracranial pathologies due to head injury was evaluated and outcome assessed at discharge. There were 95 children with EDH and 8.4% had poor outcome (vegetative state or death). There were 85 patients with contusion and poor outcome was noted in 18.8%. One hundred patients had diffuse cerebral oedema on CT scan and outcome was poor in 25% of these patients. The clinical features associated with poor prognosis were, absence of ocular movements (50%), abnormal pupillary size and reaction (49%) and age less than 2 years (27%). Key Words: Head injury, Glasgow coma scale, Children. Head injury in children forms a major subset of trauma patients.1,2 The outcome in these patients is distinctive because of the unique biophysical properties of the child's skull and brain.3 The factors affecting the outcome in children with head injuries have been studied by various authors.4,5 Several studies have highlighted the importance of age and clinical factors such as GCS (post resuscitation) score, ocular movements, pupillary size, etc. in the prediction of outcome in these patients.4-8 However, the outcome in these studies varies widely with a mortality ranging from 9% to 75% (in severe head injury).7 The present study was undertaken with a view to determine the outcome and analyze factors affecting the outcome in children with head injury. Materials and Methods Three hundred and forty consecutive children with head injury, fifteen years or less in age were managed in the Department of Neurosurgery, NIMHANS, from January 1993 to December 1998. The patients were evaluated neurologically by the best Glasgow Coma Score (following resuscitation where necessary), and its modification for children below 2 years of age (Table 1), pupillary reaction and ocular movements. They were divided into four categories depending upon the level of sensorium: GCS of 13-15, 9-12, 6-8 and 3-5. Based on brain stem reflexes, patients were grouped into two divisions: normal or abnormal signs for both pupils and ocular movements. All patients underwent plain CT scan of head with bone windows. CT scan findings noted were fractures (linear / depressed), extradural hematoma, contusion, diffuse brain injury and acute subdural hematoma. The outcome of all these patients were assessed by Glasgow outcome scale and divided into two categories: good (good recovery, moderate disability and severe disability) and poor (vegetative state and death) outcome. This was because various studies have shown that most patients with severe disability on discharge ultimately improve on follow-up at 6 months to moderate disability or good recovery.9,10 Outcome was assessed in relation to the clinical features such as age, pupillary reaction and size, ocular movements and imaging features such as fracture, extradural hematoma, contusion, diffuse head injury, and acute subdural hematoma. Results All patients were fifteen years of age or below. Of the 340 children, there were 11 children less than 2 years and 329 were above 2 years of age (Table 2). Poor outcome was seen in 27.2% children below 2 years, 16.9% in 3-5 years group, 15% in 11-15 years group. Thus children less than 2 years of age had a relatively worse outcome, but it was not however statistically significant (p = 0.74). The best GCS response after resuscitation was considered and GCS was found to be a good indicator of outcome (Table 2). There were 41 patients in GCS of 3-5, of which 24 (58.5%) had a poor outcome; while out of 51 patients of GCS 6-8, 18 (35.2%) had poor outcome. Out of 96 patients in GCS 9-12, 11 had poor outcome. There were 3 children below 2 years of age in this category which was their best score (maximum score for children below 2 years of age is 11-Table 1) and who had good outcome as expected. 2 patients with GCS of 13-15 (1.3%) had a poor outcome; of them, one had an EDH and had deteriorated before surgery, while the other had multiple associated injuries like fracture femur, hypotension, etc. Pupillary size and reaction was found to be a good indicator of outcome (Table 2). Sixtynine patients had abnormality of pupillary size and reaction, poor outcome was seen in 49.3% in contrast to only 7.4% with normal pupillary response, which was statistically significant (p<0.001). Ocular movement was found to be a good predictor of outcome (Table 2). Seventy-seven children had abnormal ocular movements, poor outcome was seen in 38 patients (50%). Among the children with normal ocular movements poor outcome was seen in 6% cases. There were 34 patients with acute subdural hematoma, 55 patients had contusion, fractures were seen in 56 patients, extradural hematoma in 95 patients and diffuse head injury in 100 patients. Outcome was found to be different in these groups. Poor outcome was noticed in 5.4% patients with fracture, 8.4% with extradural hematoma, 18.2% with contusion, 25% with diffuse head injury and 35.3% with acute subdural hematoma. Discussion The special attributes of the pediatric skull and brain accounts for their outcome being different than in adults.12 The pliability of the immature skull of newborn makes the brain more vulnerable to injury; the lack of adequate subarachnoid space reduces its buffering capacity for external applied impact.12 The immature brain appears to tolerate anoxia and hypoxia better than adults.13 Cerebral perfusion pressure is lower in children because of low blood pressure. The pediatric brain forms less edema fluids and can clear any edema more rapidly than an adult brain. Important functional differences in neuroplasticity exist in infants and young children compared with older children and adults, as myelin increases plasticity decreases.14 However in infants and very young children, young children suffer greater damage from diffuse injury than their older counterparts and show significant impairment in cognitive and performance potentials due to injury to developing brain. The higher mortality in the 0-4 years age group can be explained by the correspondingly higher incidence of subdural hematomas, bilateral non-reactive pupils and hypotension in these patients.15 There is no significant difference in outcome in pediatric and adult patients with mass lesions.16 Cumulative mortality increased up to 62% by one year for children under four years age. The importance of age as a prognosticating factor has been the subject of controversy. Luerssen, et al.17 have reported age itself as a major independent factor affecting outcome. In the present study we did not find significant contribution of age per se for outcome of head injury. Those patients in coma with a GCS score of 8 or less have a significant probability of death or major neurological deficits. Decerebration carries 60% mortality.14 A disproportionate number of children who have GCS score in the 3-5 range either die or persist in vegetative state whereas a higher proportion of children with GCS in 6-8 range attain a good recovery. Despite the relation between the depth of the coma and outcome, a wide range of GCS scores among children with good recovery exists.5 Lai-Choo Ong quoted that low GCS did not always accurately predict the outcome in absence of hypoxia or ischaemia; in our cases we have found a significant impact of GCS on outcome. Harold et al stated that pupillary response is not a good predictor of outcome.14 If the vestibulo-ocular reflex is absent there is 100% mortality and if impaired then a poor predictor of outcome. Levin et al5 described the main effects of GCS and pupillary reactivity and their interaction. In our study, about 50% of the children with either abnormal pupillary reaction or abnormal ocular movements had poor outcome. The extent of a skull fracture is proportional to severity of brain injury clearly does not apply to the pediatric age group.14 The probability of associated intracranial hematoma with skull fracture in children is half of that of adults.18 94.1% of patients with skull fracture had good outcome in our series. Extradural hematoma (EDH) is significantly less common in children than in adults and is even more rare in infants.19 EDH can occur without fracture in children more commonly.14 EDH was seen in only 6% cases by Tomberg et al.20 Unlike in other series we observed very high incidence of EDH in children (28%) and good outcome was seen in 91.6% cases. In our series the mortality in cases with EDH is lower than in other lesions. This has been seen by others as well.20 The mortality rate in children with EDH ranged from 7-15%, 5-10% of patients also had residual neurological deficits.14 Contusions were seen in 5% of cases. The outcome was unfavorable in patients with intracerebral hematomas and hemorrhagic contusions.20 In our series 18.8% of the patients with contusion had poor outcome compared to 14.9% patients without it. Diffuse brain swelling occurs in approximately 50% of children with severe head injury. The outcome is significantly better in children as compared to patients with operable mass lesion.20 Diffuse swelling of brain may develop more readily in children because of the lack of CSF available for displacement. Children with CT scan indicating of diffuse axonal injury but without diffuse cerebral edema generally did not have sustained increased intracranial pressure and more than two-thirds attained a favorable outcome. Diffuse brain swelling with or without diffuse axonal injury demonstrated by the first CT scan was related to high mortality. Thereafter the multifocal brain edema seems to occur and secondary increase in intracranial pressure is found. If these are controlled, useful recovery will occur in 80% of these patients. The outcome in patients with diffuse head injury (25%) was poor. SDH is seen six times more often in the infants than in toddlers.14 The outcome of patients with SDH is significantly worse than that of patients with EDH, mainly because of the underlying brain damage accompanying SDH and the resultant intracranial hypertension. 17.1% of the patients of Tomberg's series had SDH and none of them had good recovery.20 34.6% of the patients with SDH had poor outcome in our series in comparison to 14.3% patients without SDH or with other lesions. Although relatively poor outcome was seen more frequently in children under two years age, it was not found to be statistically significant. GCS, pupillary reaction and ocular movements were very significant predictors of outcome. With increasing order fracture, EDH, contusion, diffuse head injury and acute SDH had poor outcome. Overall poor outcome was seen in 15.8% of 340 children with head injury. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03002t2.jpg] [ni03002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}