 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 19-21 Hemodynamic response to skull pins application in children: Effect of lignocaine infiltration of scalp P. Bithal, H. H. Dash, N. Vishnoi, A. Chaturvedi Department of Neuro-anaesthesia, Neurosciences Centre, All India Institute of Medical Sciences, New Delhi-110029, India.
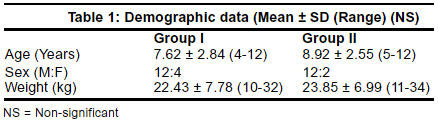
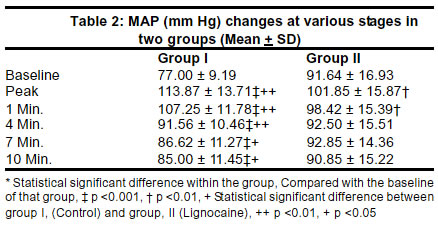
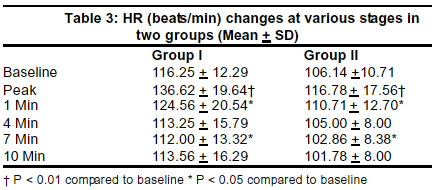
Accepted on 20.08.2001. Code Number: ni03003 Background: Skull pins application following local anesthetic infiltration of scalp obtunds hemodynamic changes in adults. No such study is available in children. Methods: 30 children undergoing elective suboccipital craniectomy with skull pins fixation, were randomly allocated either to control group I, or lignocaine group II. Whereas in group I, pins were applied without any scalp infiltration. In group II, pins were applied 1 min. after scalp infiltration with 0.5% lignocaine (plain) at each pin site. Results: Mean arterial pressure and heart rate were recorded during pinning (peak increase),1,4,7 and 10 min later, and were compared with the baseline (parameters recorded approximately 20 min. after intubation). Mean arterial pressure in group I peaked from 77.0 ± 9.19 to 113.87 ± 13.7mmHg (P<0.001) and remained significantly high throughout the study period. In Group II peak increase in mean arterial pressure was from 91.64 ± 16.39 to 101.85 ± 15.87 mmHg (P<0.01) and remained high till 1 min. only. Pins placement resulted in significant increase in heart rate only during pinning (peak increase) and up to 1 min. in both the groups (P<0.01). Conclusions: In children, skull pins placement 1 min. after scalp infiltration with 0.5% lignocaine plain fails to prevent the hemodynamic changes arising during pins placement (peak change) and up to 1 min. after pins placement. However, the technique successfully blocks these changes beyond 1 min. post skull pins fixation. Key Words: Neurosurgical anesthesia, Pediatric, Local anesthetic infiltration, Skull pin head-holder. A skull pin head-holder frequently used for intracranial procedures offers the neurosurgeon the advantages of maintaining the stability of the head of the patient and if needed, to maneuver the head position intraoperatively. The device consists of a C-shaped metallic frame and has 3 sharp pointed metallic pins which are driven manually through the skin, muscles and periosteum into the outer table of the skull until they press firmly into it in the anesthetized patient. This stimulates the scalp and periosteal nerve endings resulting in acute increase in blood pressure (BP) and heart rate (HR), despite apparently adequate depth of anesthesia, in an otherwise healthy patient.1-3 These hemodynamic disturbances may last for two minutes3 at least and may increase the incidence of morbidity in patients, particularly if there is underlying cerebrovascular pathology, viz., arteriovenous malformation (AVM) and intracranial aneurysm.4 Intracranial hemorrhage caused by brain tumour has been reported in children.5 By infiltrating the scalp with a local anesthetic to block nerve endings one would anticipate that this hemodynamic response would be prevented or blunted. In adults this technique has been shown to decrease significantly the anticipated hemodynamic response to scalp pinning.2,3 The effects of this technique for pin application in children have not been demonstrated previously. The purpose of this study was to compare the blood pressure and heart rate response to scalp pins application, with and without local anesthetic infiltration of scalp at the pin sites in children. Methods After approval from the hospital ethics committee, 30 children (ASA I/II), age below 12 years, scheduled to undergo elective suboccipital craniectomy which required the application of skull pin head holder, were studied prospectively. Informed consent was taken from the parents of the children. All the children fasted for 6 to 8 hours. One hour prior to induction, they all received promethazine (0.5 mg/kg) by intramuscular route. A standard anesthesia technique was used. The children were induced with thiopentone 5-6 mg/kg, and tracheal intubation was facilitated with pancuronium 0.1 mg/kg. Anesthesia was maintained with 66% Nitrous Oxide in oxygen. Pethidine I mg/kg IV was administered for intraoperative analgesia. Lungs were hyperventilated mechanically using Air Shield's ventilator and a Bain's circuit. Ventilation was adjusted to achieve an end tidal carbon-dioxide of 30mmHg (monitored with Datex Multicap). At this stage halothane 0.5% inspired concentration, was added to the anesthesia mixture. A 22 G cannula was inserted into a dorsalis pedis or radial artery and connected through a saline filled tubing to Gould P 35 transducer. The latter was placed at the mid axillary level for direct monitoring of BP with the help of Mennen Multichannel Horizon monitor 2000 which was set to store data at 1 minute interval. In both the groups, baseline mean arterial pressure (MAP) and HR was recorded when the patients became hemodynamically stable (approximately 20 min. after intubation). In group I these parameters were recorded just before pins application and in group II just before scalp infiltration. Patients were subsequently randomly assigned to one of the two groups with the help of random chart. In group I (16 patients) pins were applied without the use of any scalp infiltration. In group II (14 patients), the skin, subcutaneous tissues, and periosteum was infiltrated at each site for pin placement, with 0.5% lignocaine (5mg/ml), without epinephrine, using 2ml at each site. One minute was allowed to pass before pins were tightened into the skull. MAP and HR recordings were made at the following intervals: during skull pinning, (peak rise), at 1,4,7 and 10 min. post pins application. Since MAP and HR increase abruptly over a period of few seconds during tightening of pins, to determine the peak increase in these parameters each reading of increase in their values was stored manually in the monitor until such time there was no more increase. At the end of the study, the stored data was reviewed and the peak rise in MAP and HR was noted for the purpose of analysis. Hemodynamic changes in response to pin fixation were compared with the baseline in each group. Also the hemodynamic parameters at each step of recording were compared between the two groups. Statistical analysis: Descriptive statistics for MAP in both the groups was done by mean and standard deviation. Since the baseline values for MAP were statistically different in the two groups, percentage changes were calculated at each of the subsequent times. In order to detect a significant change from baseline within the same group, Wilcoxon sign rank test was applied. To compare average MAP changes in between the groups, at each point of time, Wilcoxon rank sum (Mann-Whitney) test was applied due to non-normality of distribution of percent change in values. P value of less than 0.05 was taken as statistically significant. Paired `t' test was applied to compare changes in mean HR from baseline in each group separately. Wilcoxon rank sum test (Mann-Whitney), was used to compare differences in HR in the two groups at each point of time. P value of less than 0.05 was taken as statistically significant. Chi square test and student's `t' test were applied to compare the demographic data of the two groups. P value of less than 0.05 was taken as significant. Results A total of 30 patients were studied. Group I consisted of 16 patients whereas group II had 14. The two groups were well matched for age, sex and weight (Table 1). All the data are reported as Mean + SD. In group I skull pinning increased MAP significantly from77.00 ± 9.19 mmHg to 113.87 ± 13.71 mmHg (P<0.001) and this significant increase in MAP was observed at each point of recording throughout the study period (Table 2). In group II also pinning resulted in significant increase in MAP from 91.64 ±16.39mmHg to 101.85 ± 15.87 mmHg (P<0.01), however, this significant increase lasted only till 1 minute following pinning (Table 2). Inter-group comparison showed significant increase in MAP in group I at each step of recording (Table 2). In group I pins resulted in significant increase in HR from 116.75 ± 12.29 to 136.62 ± 19.64 beats per min (P<0.01). This increase in HR lasted only upto 1 min. post pins application and subsequently it started to decline, being significantly less (P<0.05) compared to the baseline at 7 min. In group II also there was significant increase in HR during pinning from 106.14 ± 10.71 to 116.78 ± 17.56 beats per min (P<0.01), and this increase too lasted only up to 1 min. post pins fixation. Inter-group comparison of HR showed comparable changes at each step of recording (Table 3). Discussion Scalp pins application resulted in significant increase in MAP in both the groups. In Group I, this increase in MAP continued till 10 min. post pins fixation, the point at which the study was concluded. In Group II the increase in MAP was less pronounced and lasted only upto 1 min. post pins application. The hazard of acute arterial hypertension in a neurosurgical patient with potentially decreased compliance is well established and may result in increased intracranial pressure (ICP),6 especially if cerebral vessels have a limited ability to autoregulation,7 or if there is peritumoral edema.8 These observations emphasize the importance of using a technique which can blunt this response consequent upon noxious stimulus to scalp. Skull block in adults, and scalp infiltration with local anesthetic in adults as well as in children, has been recommended to blunt hemodynamic response to scalp incision.9,10,11 Similarly scalp infiltration with a local anesthetic at pin sites has been used in adults to prevent hemodynamic changes resulting from pin application.2,3 Whereas Colley and Dunn2 infiltrated the scalp at each pin site, with 2-3 ml. of 0.5% plain lignocaine, Levine et al3 used 0.5% mepivacaine with adrenaline for this purpose. In both these studies authors waited for full one minute after scalp infiltration before pin placement was permitted,and they were successful in blunting the hemodynamic consequences. However, in children we failed to reproduce the results of above studies performed in adults. In our study perhaps, the 0.5% (5mg/ml) concentration of lignocaine was ineffective and probably higher concentration could have been effective. But, resorting to higher strength of lignocaine with 2ml at each pin site, may predispose a child to lignocaine toxicity which may be impossible to detect clinically under anesthesia. In our study we used 1.4 mg/kg of lignocaine on an average in each child which is well below the upper prescribed limit. More importantly, the time interval of 1 min. between scalp infiltration and pin application was probably insufficient to blunt the hemodynamic response. The latter hypothesis seems more likely and gets support from the observation that beyond 1 min. post pin fixation, there was no increase in MAP in group II. Retrospectively we speculate had we waited for at least 2-3 min. after the scalp infiltration this hypertensive response could probably have been blunted. However, this needs further studies. Infiltration of scalp with local anesthetic is a simple and safe technique to blunt the hemodynamic changes. This technique circumvents the need to control BP with a vasodilator, and the need for increasing an anesthetic depth with a volatile agent, all of which take time to initiate, and at times may induce hypotension, increase in cerebral blood flow and unacceptable increase in ICP10 which may result even when isoflurane is used, despite modest hyperventilation.12 In summary, skull pins application in children, one minute after scalp infiltration at each pin site with 2cc 0.5% lignocaine (without adrenaline), is ineffective in preventing hemodynamic change. The appropriate time interval to obtund hemodynamic changes needs further studies. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03003t1.jpg] [ni03003t2.jpg] [ni03003t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}