 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 22-26 Incidence of intracranial aneurysms in northwest Indian population K. Kapoor, V. K. Kak* Department of Anatomy, Govt. Medical College, Chandigarh-160 030, India. and *Department of Neurosurgery, Postgraduate Institute
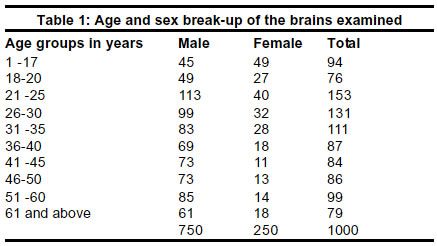
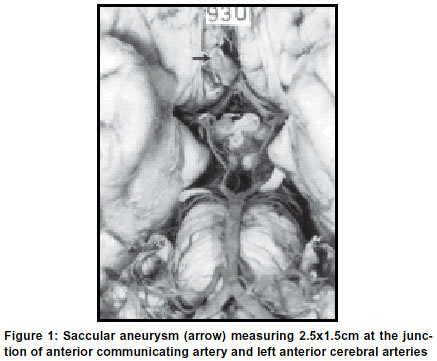
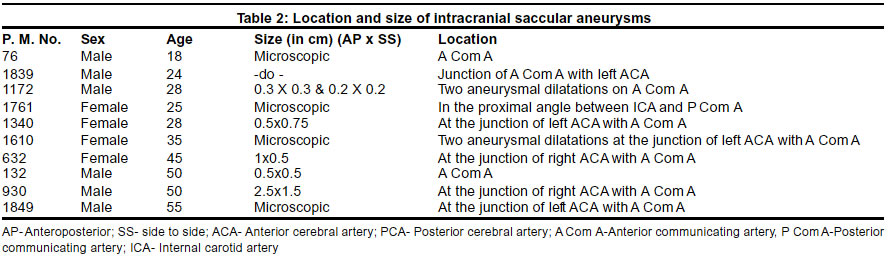
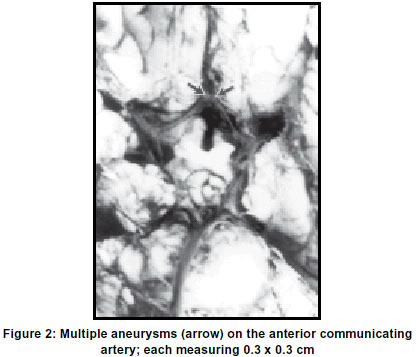
of Medical, Education and Research, Chandigarh-160012, India. Accepted on 07.09.2001. Code Number: ni03004 One thousand human brains of both sexes were examined. Aneurysms were found in 10 specimens (1%). The incidence of aneurysms was 1.6% in females and 0.8% in males. All the aneurysms were saccular. The aneurysms varied in size. In 5 specimens the aneurysms were minute bulbous dilatations. In the rest of the cases it varied from 0.2 to 2.5 cm. In 7 specimens the aneurysms were present at the junction of anterior cerebral artery with the anterior communicating artery, in 2 on the anterior communicating artery and in one specimen it was seen at the origin of posterior communicating artery. The youngest subject with saccular aneurysm was an 18-years-old male and the oldest was a 55-years-old male. No aneurysm was found in the brains of 94 children (1-17 years). Key Words: Aneurysm-intracranial, Aneurysmal dilatations, subarachnoid hemorrhage, Circulus arteriosus. The reported incidence of berry aneurysms in autopsy studies shows a wide variation in western countries,1-7 as well as various regions of India.8-10 Reddy, Prabhakar and Rao11 could not demonstrate any aneurysm in a series of 357 autopsies, whereas Tandon,12 in the collaborative study, found aneurysms in 1.8% of 185 pathological autopsies but none in 138 medicolegal autopsies. Vare and Bansal13 reported an incidence of 10.3% in 175 dissection hall cadavers from Maharashtra. Ohaegbulam et al14 reported racial differences in the incidence of aneurysms, and found whites twice more prone to having aneurysms than the black population. Locksley15 observed that the anterior communicating artery was usually the most common single site for an aneurysm, while some others4,6,16 reported the middle cerebral artery to be the commoner site. Crompton17 described that the commonest site for occurrence of aneurysm on the middle cerebral artery was at its "trifurcation". Hoffmann18 studied 75 cases of intracranial aneurysms and found 30 aneurysms on the internal carotid artery, 12 on the anterior communicating artery and 10 each on the basilar and vertebral arteries. Multiple aneurysms have been reported by several investigators.2,6,19,20 Chason and Hindman20 reported that the maximum incidence of aneurysms was between 31-70 years, finding none on the brains of 225 cadavers below the age of 20 years. However, Ostergaard21 reported an incidence of 1-3% in childhood in a "large" epidemiological aneurysm series. McDonald and Korb,22 Ask-upmark and Ingvar23 and Hamby24 reported cerebral aneurysms to be commoner in females than in males. There are reports that aneurysms are more common on the left than the right side,23,25,26 but contrary observations have also been reported.3,4,27 Ramamurthi28,29 noted that the incidence of aneurysms on either side was "almost equal". It was therefore considered worthwhile to undertake an investigation on a large series to determine the incidence of intracranial saccular aneurysms in relation to their size, site, sex and age in north-west Indian population and to see if any differences exist in comparison to the western population. Material and Methods One thousand brains from cadavers were obtained from medicolegal autopsies performed by the Anatomy Department, P.G.I., Chandigarh. Brains were removed from the skulls and fixed in 10% formalin for a minimum period of one week. The circle of Willis at the base of the brain was examined. All arteries were closely examined with the aid of a magnifying lens and, if necessary, under a dissecting microscope to ascertain the presence of one or more aneurysms. If an aneurysm was present, the age and sex of the subject and its location was recorded. The size of the aneurysm was measured with a caliper. The age and sex break-up of the brains examined is given in Table 1. Results Ten out of the 1000 brains studied showed the presence of aneurysms giving an incidence of 1%. The aneurysms could be seen by the naked eye in five specimens (Figure 1), while in the remaining five, the aneurysms were small and could be observed with the help of a hand lens or under a dissecting microscope. The location and sizes of all the aneurysms, along with the age and sex of the subjects, are listed in Table 2. The ages of subjects having aneurysms ranged from 18 to 55 years. No aneurysm was found below the age of 17 years (94 specimens) and above the age of 56 years (126 specimens). Aneurysms were seen in 6 out of 750 (0.80%) male subjects and 4 out of 250 cases (1.60%) female subjects. There were 2 specimens with two small aneurysms each present on the anterior communicating artery (Figure 2). All the aneurysms were present in the anterior half of the circle of Willis. Seven were located at the junction of the anterior communicating artery with the anterior cerebral arteries (Table 2), 4 on the left and 3 on the right side. In 2 specimens the aneurysms were seen on the anterior wall of the anterior communicating artery about its middle. In one instance the aneurysm was present in the medial angle between the right internal carotid and the origin of the posterior communicating artery. In one specimen, one of the aneurysms was present in the distal angle between the right anterior cerebral and anterior communicating arteries, while the other was present adjacent to it projecting from the anterior wall of the anterior communicating artery. In the other specimen too, the aneurysms were present in a similar position but on the left side. Discussion The incidence of aneurysms has variously been reported as 0.25%,1 1.5%,30 0.8%,6 0.87%,16 0.5-1%,24 5.6%4 and 22%.31 Riggs and Rupp,2 in a study of 1,437 brains, found aneurysms in 9% specimens. However, in a consecutive study of 13,219 autopsy brains, Walton27 discovered aneurysms only in 0.93% instances. A planned autopsy study of 2,786 autopsy specimens reported the incidence of berry aneurysms as 4.9%.20 In India, the incidence of intracranial aneurysms from Chandigarh was given as 4.5% by Banerjee8 in pathological autopsy brains. In a subsequent study from the same centre, the incidence was reported as only 2%.9 An ICMR collaborative study found only one specimen showing an aneurysm in 81 pathological autopsies.12 Ramamurthi28 had reported that berry aneurysms were rare in south Indian subjects (0.75%). Reddy et al11 did not find a single aneurysm in 357 medicolegal autopsies at Hyderabad. Vare and Bansal13 reported the incidence of aneurysms as 10.3% in brains obtained from dissection hall cadavers in Maharashtra. Their figures were higher than those of other Indian workers and many of the western authors. In the present series, intracranial aneurysms were found in 10 out of 1,000 specimens examined (1%). This incidence is almost similar to that reported by Inagawa and Hirano6 Hamby,24 Walton27 and Osler.30 Aneurysmal size has been reported in the literature by some workers. Riggs and Rupp2 found aneurysm size to be less than 0.5 cm. Inagawa and Hirano6 in a study of 10,259 autopsies from 1951 to 1987, reported that 54% of the aneurysms were 4 mm or less and 35% were 5-9 mm in size. Chason and Hindman20 reported the average size of ruptured aneurysms to be 8.6 mm, as compared to 4.7 mm of unruptured ones. They did not find any significant correlation between sex and size of an aneurysm. Dinsdale32 described very small aneurysmal dilatations, measuring only 0.2-1.0 mm. Banerjee9 observed 2 out of 4 specimens having an aneurysm to be saccular, measuring 1 cm in size. The aneurysm in the third specimen was also saccular but could be seen only under the microscope, while the fourth aneurysm was mycotic and measured 0.5 mm. In the present investigation there were 10 specimens of saccular aneurysms, half of which were seen by the naked eye while the other five could be observed only by a hand lens or under a dissecting microscope. In 3 specimens, the aneurysm size varied between 0.2-2.5 cm, while one of the aneurysm was large measuring 1.5 cm side to side and 2.5 cm anteroposteriorly (Figure 1). Most workers have reported over 75% of the saccular aneurysms to be located in the anterior half of the circle of Willis. Hoffman18 found 40% aneurysms on the internal carotid artery, 16% on the anterior communicating and 6.6% each on the basilar and vertebral arteries. McDonald and Korb22 reported 48% aneurysms on the internal carotid artery, 15% on the anterior communicating and 28% posterior to the internal carotid artery. Seventy-five per cent of aneurysms were located at the junction of anterior cerebral with anterior communicating artery in the brains examined by Riggs and Rupp,2 the posterior half of circulus arteriosus was involved in only 13% brains. However, Housepian and Pool33 reported 23% aneurysms at the junction of anterior cerebral and anterior communicating arteries, while 41% were located on the internal carotid, 33.5% on the anterior cerebral, 19.8% on the middle cerebral, 2.9% on the basilar and 0.9% on the vertebral arteries. Chason and Hindman20 reported 90% aneurysms in the anterior half of the circle of Willis, out of which the anterior communicating artery was involved in 35% specimens. Brust34 also reported similar observations. Walton,27 in his book on subarachnoid hemorrhage, compared the location of intracranial aneurysms in his series with that given by McDonald and Korb.22 While the percentage of aneurysms present in the anterior half of the circle of Willis was almost similar, the reported incidence in the posterior half was much lower than that in the cases reviewed by the latter. He was of the opinion that some of the earlier so-called basilar aneurysms could be syphilitic. He further stated that "undue preponderance" of aneurysms of internal carotid artery in some series24 might be due to the fact that it is easier to locate an aneurysm in this situation. Stehbens4 found 88.7% of the aneurysms in the anterior half and only 11.3% in the posterior half of the circle of Willis. In India, Vare and Bansal13 reported 67% of aneurysms on the anterior cerebral artery, 22% on the basilar artery and 10% on the posterior cerebral artery. Banerjee9 found all four aneurysms in his report in the anterior half of the circle of Willis. The aneurysms were present on the anterior communicating artery in 2 specimens, while the middle cerebral artery was involved in the other two. Ramamurthi29 reported 35% aneurysms on the internal carotid artery, 30% on the anterior cerebral and communicating arteries and only 10% in the posterior half of the circle of Willis. Sambasivan et al10 observed 38.5% aneurysms on the supraclinoid part of the internal carotid artery at the origin of the posterior communicating artery, 31% on the anterior cerebral artery, 17% on the middle cerebral artery and only 1.7% on the basilar and posterior cerebral arteries. In the ICMR collaborative study on subarachnoid haemorrhage, Tandon12 reported 45.9% aneurysms on the internal carotid artery, 24.8% on the anterior communicating artery, 17% on the middle cerebral artery, 10% on the anterior cerebral artery and only 1.08% on the posterior half of the circle of Willis. All the aneurysms in the present study were located in the anterior half of the circle of Willis. The aneurysms were located at the junction of the anterior cerebral and anterior communicating arteries in 7 specimens, on the anterior communicating artery in 2 and at the origin of the posterior communicating from the internal carotid artery in 1 specimen. Williams et al3 and Hamby24 reported aneurysms to be commoner on the right side, but contrary observations were made by Gower.25 McDonald and Korb,22 Wells26 and Walton27 did not find any significant side differences. Amongst the Indian workers, Vare and Bansal13 reported more aneurysms on the right side, but Banerjee9 and Ramamurthi28 did not observe any difference between the two sides. In the present series also the aneurysms were distributed equally on either side. Several investigators have reported cerebral aneurysms to be more common in females than in males.22-24 Chason and Hindman20 found the incidence of berry aneurysms to be 3.5% in males and 7.2% in females. Locksley15 also reported that females were twice more prone to have aneurysms than males, the ratio being 2.4:1. Stehbens4 reported 252 subjects with cerebral aneurysms, which included 52.4% women and 47.6% men. Some Indian workers10,13,28,29 have not mentioned the sex incidence of aneurysms. In the present investigation, a total of 750 male and 250 female brains were examined. Saccular aneurysms were found in six (0.8%) male and four (1.6%) female brains; the ratio being 1:2. These observations are similar to those reported in the literature. Riggs and Rupp2 did not find even a single aneurysm in a group of 102 infants and children under 10 years of age. According to them, they had confirmed Forbus's theory that these aneurysms were not congenital but related to structural defects. Chason and Hindman20 similarly failed to locate any aneurysm under the age of 20 years. The incidence was maximum in the age group of 31-70 years, with a mean age of 57 years. Stehbens4 calculated the mean age of subjects with cerebral aneurysms as 50.2 years. Similarly, there was a low incidence of aneurysms in the age group above 70 years. Walton,27 however, has given the age incidence higher than that of the above mentioned authors but, as he explained, all the cases in his series had ruptured aneurysms. Ramamurthi29 stated that in the Indian population, aneurysms were most commonly found between the ages of 40-60 years. Tandon12 reported only 2.2% aneurysms under the age of 20 years, while an incidence of 19.4% was observed in subjects above the age of 60 years. The remaining 79% of cases were found between the ages of 20-59 years. In the present investigation, the youngest subject with a saccular aneurysm was an 18-year-old male and the eldest was a male of 5 years. No aneurysm was found in the age group of 1-17 years and above 55 years. While inability to find any aneurysm in the younger age in our series is in conformity with the earlier reported observations, one of the reasons for failure to locate any aneurysm in the older generation might be the fact that the present study had a lesser number of cases in this age group as compared to the middle age groups. Multiple aneurysms in a single brain have been reported by several western workers, the incidence varying from 8.3 to 33.3%.2,4,5,19,20,27 Tandon12 reported the presence of 185 aneurysms in a total of 180 patients of subarachnoid hemorrhage. It was,however, not clarified as to how many subjects had more than one aneurysm. In the present material multiple aneurysms were found in 2 subjects (20%). In each instance there were two aneurysms situated side by side on the anterior wall of the anterior communicating artery. The aneurysms were very small and could not be seen well with the naked eye. These observations are nearly the same as those reported by Stehbens4 and Chason and Hindman.20 The incidence of intracranial arterial aneurysms from various parts of India varies from 0.75 to 10.3%8,9,12,13,28 while that reported from western countries varies from 0.25 to 22%.1,4,16,24,30,31 Aneurysms were found in 0.8% of 10,259 Japanese6 and 8.5% of 310 Ghanaian normotensive subjects,7 while the north-west Indian population in the present study had an incidence of 1%. Due to the wide variations in published reports, it is not possible to conclusively support the observations that Asian and African countries have a lower incidence of aneurysms as compared to their European counterparts.14,28 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03004t2.jpg] [ni03004f1.jpg] [ni03004t1.jpg] [ni03004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}