 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
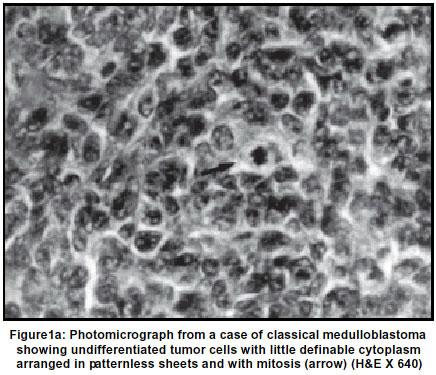
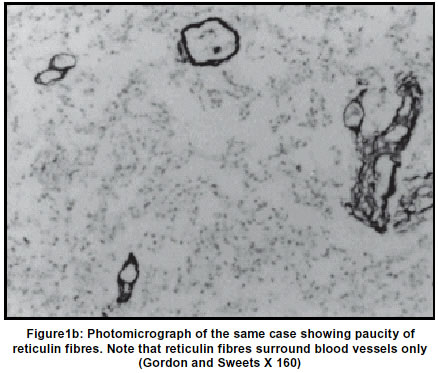
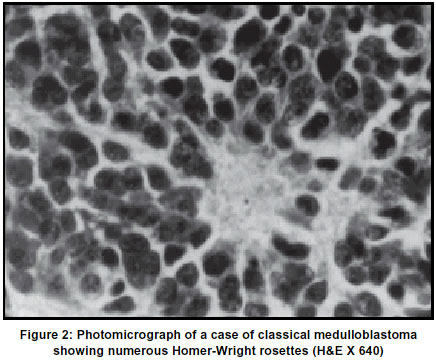
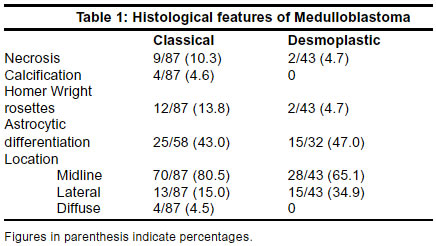
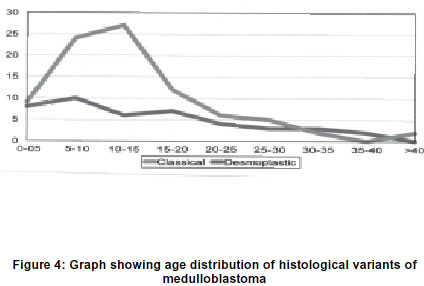
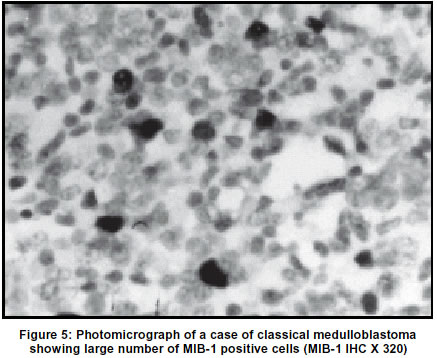
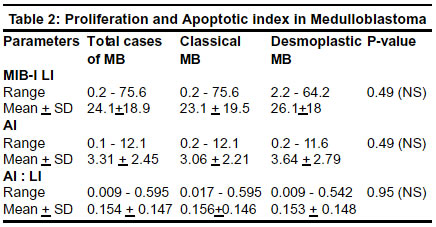
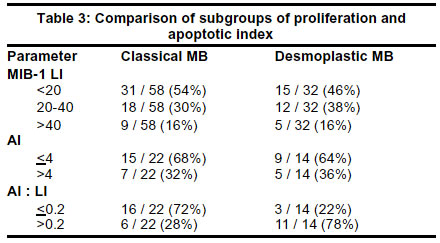
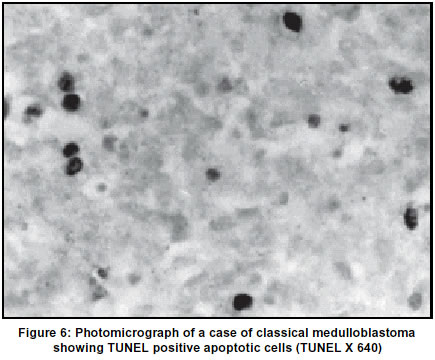
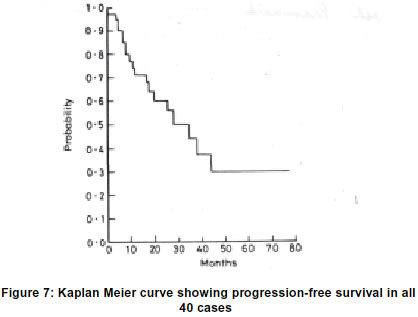
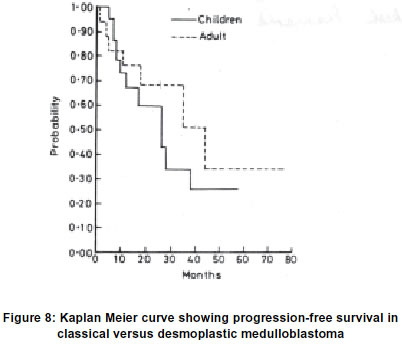
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 27-34 A comparative study of classical vs. desmoplastic medulloblastomas P. Pramanik, M. C. Sharma, P. Mukhopadhyay,# V. P. Singh,* C. Sarkar Departments of Pathology, #Radiotherapy and *Neurosurgery, All India Institute of Medical Sciences, New Delhi, India. Accepted on 12.11.2001. Code Number: ni03005 Classical and desmoplastic medulloblastomas (MBs) have been suspected to be biologically different, though comparative studies on markers of biological aggressiveness in these two variants are sparse in the literature. 87 classical and 43 desmoplastic variants of MB were studied with respect to clinical and histological characteristics, MIB-1 labeling index (MIB-1 LI), apoptotic index (AI), ratio of AI to MIB-1 LI, expression of p53 and Bcl-2 protein and 3-year progression-free survival. The only differences documented between the variants were with regard to age distribution and location. Thus, classical histology cases occurred predominantly in children and 80% were midline in location. In contrast, lateral location was seen more frequently with tumors of desmoplastic histology, which occurred in an almost equal distribution between children (56%) and adults (44%). No difference was noted between the variants with regard to proliferation index, apoptotic index, their ratio on or their molecular controls (p53 and Bcl-2). This was reflected in the clinical outcome wherein no significant difference was observed in the 3-year progression-free survival between the variants. It is concluded that the two histological variants of medulloblastoma are not different with regard to biological parameters of aggressiveness. The growth rate and clinical outcome in medulloblastomas have no correlation with the histological variant. Key Words: Medulloblastoma, Histology, MIB-1 labeling index, Apoptotic index, Bcl-2 protein. Medulloblastomas have long been classified into two chief histological variants, "classical" and "desmoplastic".1-4 Other variants of medulloblastoma - large cell, lipomatous, melanocytic and medullomyoblastoma are rarer.3,4 Available literature reports have documented some differences between classical and desmoplastic medulloblastomas with regard to age of occurrence, location, cell of origin, glial/ neuronal differentiation and DNA content, thus prompting the view that the variants may indeed be different.2,4-14 Further, desmoplastic medulloblastomas were initially thought to carry a more favorable prognosis than the classical variant but this belief has been subsequently refuted.15-20 However, studies on biological parameters of aggressiveness, namely proliferation, apoptosis and their molecular controls in classical versus desmoplastic medulloblastoma are very few.21-23 In the present study a comparative evaluation of 87 cases of classical and 43 cases of desmoplastic medulloblastomas have been done in terms of (a) clinical parameters (b) histological parameters (c) astrocytic differentiation (d) proliferation rate [MIB-1 labeling index] (e) apoptotic index (f) ratio of apoptosis to proliferation and (g) expression of proteins of two genes controlling tumor growth rate, namely p53 tumor suppressor gene protein and Bcl-2 protein. Materials And Methods The total number of intracranial tumors diagnosed in the Department of Pathology, All India Institute of Medical Sciences over a 10- year period (1989-1998) both in children (age <15 years) and in adults (age >15 years) were obtained from the records. Posterior fossa tumors were then selected out and histological diagnosis noted in each case. Subsequently, from the posterior fossa tumors, all cases of medulloblastoma diagnosed during this 10-year period were selected. Retrospective histologic material was jointly reviewed in each case and a concordant agreement established for the diagnosis. Thus, in a total of 181 cases of medulloblastoma obtained from the records during the 10-year period, the diagnosis was reconfirmed. Clinical data were obtained from the Depts. of Pathology and Neurosurgery. One representative block of formalin fixed paraffin embedded tissue was selected for each case. 10 serial five micron thick sections were cut from the block and 3 sections taken on ordinary albumin coated slides while the remaining 7 were taken on poly-L-lysine coated slides (M/s. Sigma, USA). The following stains were done - haematoxylin and eosin (H&E) stain (n=181); reticulin stain (Gordon and Sweet's Silver Impregnation Method) (n=130); immunohistochemical stain by the Streptavidin-Avidin-Biotin immuno-peroxidase technique (LSAB) using monoclonal antibodies to glial fibrillary acidic protein (GFAP), MIB-1 (n = 90), p53 protein (DO-1) and Bcl-2 protein (n=90); Terminal deoxynucleotidyl transferase dUTP mediated nick end labelling (TUNEL) technique for apoptotic cells (n=36). For the various stains including the four immunostains, there was no selection bias and they were all consecutively operated upon cases. The only selection criteria were availability of paraffin blocks and presence of adequate tissue in the block. For TUNEL technique, in addition to the availability of adequate tissue in the block after the immunostains had been done, the other limiting criterion was the availability of reagents in the TUNEL kit after standardization of the procedure. Immunostaining method for gfap, mib-1, p53 and bcl-2Sections were deparaffinized (2 changes of xylene x 5 minutes each, 1 change of acetone x 1 minute) followed by rehydration in decreasing ethanol concentration (95% ethanol x 3 min., 70% ethanol x 3 mins., distilled water x 1 min.). For MIB-1, p53 and Bcl-2 immunostaining, the tissue sections were then subjected to high temperature microwave antigen unmasking by heating the sections immersed in 10 mM citrate buffer pH 6.0 (prepared by dissolving 2.1 gm. of anhydrous citric acid crystals in 1 litre of distilled water and pH adjusted to 6.0) inside a 600-watt microwave oven in full power for 35 min. The slides were allowed to cool to room temperature and then washed briefly with 0.05 M Tris HCl buffer, pH 7.4. For GFAP immunostaining however, no antigen retrieval technique was applied. To diminish non-specific staining (endogenous peroxidase activity), each slide was treated with methanol containing 3% hydrogen peroxide (H2O2) for 30 min. (1 part 3% H2O2 + 4 parts absolute methanol). After brief rinsing, the sections were placed in 0.05 M Tris HCl buffer pH 7.4 for 10 min. Excess buffer was tapped off followed by careful wiping around the specimen. Sections were then overlaid with adequate amount of appropriately diluted primary antibody followed by overnight incubation at 4°C in humid chamber. MIB-1 antibody was obtained from M/s Immunotech, USA, and was used in a dilution of 1:250. p53 antibody (DO-1) was used from M/s Santacruz, USA and the dilution was 1:100. GFAP and anti Bcl-2 antibodies were obtained from M/s Dako Patts, Denmark and were used in a dilution of 1:500 and 1:40 respectively. The slides were then washed in 3 changes (5 min. each) of 0.05 M Tris HCl buffer, pH 7.4 followed by incubation for 30 min. at room temperature after application of biotinylated secondary antibody of anti-mouse (anti-rabbit) immunoglobulins in phosphate buffered saline containing carrier protein and 15 mM sodium azide (Large volume universal DAKO LSAB kit, Peroxidase, M/s Dako Patt, Denmark). After 3 washings (5 min. each) in Tris HCl buffer, peroxidase conjugated streptavidin was applied to cover the specimens and incubated at room temperature for 30 min. Slides were rinsed with 3 changes of Tris HCl buffer 5 min. each. Sections were then covered with substrate chromogen solution prepared freshly by dissolving 1 mg of 3,3' diaminobenzidine tetrahydrochloride or DAB (M/s Sigma, St. Louis, USA) in 1 ml of 0.05 M Tris HCl buffer pH 7.4 containing 1 ml of hydrogen peroxide. The slides were incubated at room temperature for 5-10 min. under microscopic control till the optimum development of brown coloured peroxidase reactant product. After rinsing in distilled water the sections were counterstained with Harris Haematoxylin, followed by mounting with DPX as mounting media. Precautions were taken so that drying of tissue section strictly does not occur at any point of time during the entire procedure of immunostaining. All incubations were done inside the humid chamber. During each batch of staining, appropriate positive and negative controls were used. Negative controls were achieved by omitting the primary antibody. Sections from a glioblastoma multiforme, overexpressing p53 protein, were used as positive control. Sections of reactive lymphadenitis were used as positive control for Bcl-2 and MIB-1 staining. For GFAP staining, normal brain sections were used as positive control. Tunel Technique (Terminal Deoxynucleotidyl Transferase Dutp Mediated Nick End Labeling)The TUNEL technique was done using the TUNEL kit obtained from M/s Boehringer-Mannheim, Germany. The selection criteria were not only availability of adequate tissue in the block after the histological and immunostains but also the availability of reagents in the TUNEL kit after standardization of the procedure. Five micron thick tissue sections were deparaffinized and brought to water. Nuclei of the tissue sections were stripped from proteins by incubation with Proteinase K (20 microgram / ml in 10mM Tris-HCl buffer pH 7.6) for 30 minutes at 37°C. The slides were then washed in phosphate buffered saline (PBS) x 3 times. Endogenous peroxidase was blocked by covering the sections with 0.3% of hydrogen peroxide in methanol for 30 min. at room temperature. The sections were rinsed with PBS x 3 times. The sections were covered with 50 ul of TUNEL mixture and incubated in humid chamber at 37°C for 60 minutes. Washing in PBS was again done x 3 times and the area around the sample dried. The sections were then covered with 50 ml of converter peroxidase mixture and incubated in humid chamber at 37°C for 60 minutes. Washing was again done with PBS x 3 times. Sections were then covered with substrate chromogen solution prepared freshly by dissolving 1 mg of 3,3' diaminobenzidine tetrahydrochloride or DAB (M/s Sigma, St. Louis, USA) in 1 ml of 0.05 M Tris HCl buffer pH 7.4 containing 1 ml of hydrogen peroxide. The slides were incubated at room temperature for 5-10 min. under microscopic control till the optimum development of brown coloured peroxidase reactant product. After rinsing in distilled water, the sections were counterstained with methyl green followed by mounting with DPX as mounting media. Mib-1 Labeling Index (Mib-1 Li) was evaluated by immunohistochemical staining for MIB-1. The labeling index (LI) was then calculated as the percentage of labeled nuclei per 1000 cells. One thousand tumor cells were counted in several areas of tissue in which positively stained nuclei were distributed. In some cases, the MIB-1 positive nuclei were evenly distributed. But in those cases with uneven distribution of positive nuclei, the LI was generally calculated in the areas with the highest density of positive nuclei by visual analysis. This modality was less prone to errors and provided evaluation of that part of the tumor with highest growth rate. The range and mean LI values were then calculated. Apoptosis was evaluated by the TUNEL technique. Apoptosis Index (AI) was determined by counting 1000 cells and expressing it as the number of labeled cells per 1000 cells. Labeled cells adjacent to or within necrotic areas were excluded while counting apoptotic index. The range and mean AI were then calculated. Ratio of AI to Mib-1 labeling index was calculated in each case taking the AI and MIB-1 LI of the respective case. The mean AI : PI ratio was then established. Progression-free survival curves were generated by Kaplan-Meier method. The log rank statistics were used to compare the distribution of survival times between the groups (Mantle and Cox). All statistical analyses were performed using the BMDP package (BMDP: Statistical Software Inc., Los Angeles, University of California, 1983). Results A total number of 3545 primary intracranial tumors (excluding pituitary adenomas) were reported during the study period, of which 613 (17.3%) occurred in children and 2932 (82.7%) in adults. A total of 1030 (29%) of these were located in the posterior fossa. There were 181 histologically confirmed medulloblastomas, accounting for 5% (181 / 3545) of all intracranial tumors and 17.6% (181 / 1030) of all posterior fossa tumors. Out of the 181 medulloblastomas, 112 (62%) occurred in children (<15 yrs) in contrast to only 69 (38%) in adults (>15 yrs). Histological variant and other histological features were studied in 130 of the 181 cases. Out of these, 87 were diagnosed as classical histology (67%) and 43 as desmoplastic variant (33%). No case of large cell or melanotic variant was noted. Classical variant was characterized by extreme cellular density with every field being packed with small cells having high nuclear cytoplasmic ratio and frequent mitosis (Figure 1a). The cytoplasm was scanty and poorly defined while the nuclei were round, oval or carrot shaped, being variable in size and highly hemotoxyphilic, imparting a blue tinctorial quality to histological sections. These small undifferentiated cells were most commonly present in a patternless sheet arrangement (Figure 1a). Occasionally, tumor cells were arranged as pseudorosettes about the supporting blood vessels. Reticulin was absent or minimal and concentrated around blood vessels (Figure 1b). Neuroblastic differentiation as evidenced by formation of Homer-Wright rosettes (Figure 2) was present in 12/87 (13.8%) classical cases. Necrosis and calcification were rare features being present in only 9 (10.3%) and 4 cases (4.6%) respectively (Table 1). Histologically, desmoplastic variant displayed a characteristic biphasic and follicular (nodular architecture) in which compact sheets and trabeculae of undifferentiated cells surrounded pale islands of more loosely textured tissue containing cells with polar, finely fibrillated processes (Figure 3). This pattern was accentuated in preparations stained for reticulin fibres, wherein reticulin-free islands of variable sizes (corresponding to the pale islands on H&E sections) were encompassed by zones of tumor that were rich in reticulin. Neuroblastic Homer-Wright rosettes were present in only 2/43 (4.7%) cases. No case showed calcification and only 2 tumors (4.7%) had small foci of necrosis (Table 1). The mean age for cases of classical medulloblastoma was 13.4 years (range 9 months to 50 years) and that for desmoplastic variant was 14.5 years (range 1 ½ years to 40 years). It was noted that of the 87 classical medulloblastomas, 60 (69%) occurred in the childhood group with 51 of the 60 cases occurring between 5 and 15 years of age. The number of cases of classical histology declined with increasing age (Figure 4). In contrast, there was an almost equal distribution of desmoplastic cases over the entire age range (Figure 4). Thus, 24 / 43 (56%) of desmoplastic histology cases occurred in the childhood group and 19 / 43 (44%) in the adult group. Male preponderance was observed in tumors of both classical and desmoplastic histology, the male to female ratio being 2.2 : 1 and 4.3 : 1 respectively. Comparing the location of the classical vs. the desmoplastic variant, it was observed that 70 of the 87 classical histology cases (80.5%) were in the midline while only 13 (15%) were in the lateral location and 4 (4.5%) were diffuse involving both vermis and cerebellar hemispheres. However, the distribution of the desmoplastic variant was 65% (28 / 43) in the midline and 35% (15 / 43) in the lateral location respectively. Thus, the commonest site of the classical variant of medulloblastoma was in the midline. However, laterally located tumors were more frequently of desmoplastic histology. The difference in location was found to be statistically significant (p<0.05). Astrocytic differentiation was studied in 90 consecutive cases, of which 58 were classical (34 children) and 32 were desmoplastic (15 children). Evidence of astrocytic differentiation, as evidenced by GFAP immunoreactivity within the tumor was seen in 40 out of 90 cases (44.4%). Scattered reactive astrocytes were not included. Only true astrocytic differentiation represented by GFAP positive cells with nuclei resembling that of tumor cells were taken as positive. There was no difference in astrocytic differentiation between the classical and desmoplastic variants. Thus, 25/58 (43%) classical cases and 15/32 (47%) desmoplastic cases showed GFAP positive astrocytic differentiation (Table 1). Mib-1 Labeling Index (Mib-1 Li) was calculated in 90 cases of which 58 were classical (34 children) and 32 were desmoplastic (15 children). Medulloblastomas showed a high proliferative rate with the mean MIB-1 LI of all the 90 cases being 24.1±18.9 and median 20.2 (range 0.2-75.6) (Figure 5). There was no significant difference in the MIB-1 LI between the classical and desmoplastic variants (Table 2). The tumors were then further subdivided based on LI ranges but again no difference was noted between the two variants (Table 3). Thus, of the 58 classical histology cases, 31 (54%) had LI <20, 18 (30%) had LI between 20 and 40 and 9 (16%) had LI >40. Similarly, of the 32 desmoplastic histology cases, 46% (15) had LI >20, 38% (12) between 20 and 40 and 16% (5) had LI >40. The MIB-1 positive nuclei were found to be regularly distributed in classical medulloblastomas while they were absent in the central part of reticulin-free islands of desmoplastic medulloblastomas. Apoptotic cells were estimated in 22 classical (13 in children) and 14 desmoplastic (5 in children) cases. Medulloblastomas showed a high AI with mean being 3.31+2.45 (range 0.2 to 12.1) (Figure 6). There was no difference in the AI between the classical and desmoplastic variants (Table 2). On further analysis of the tumors into subgroups based on AI ranges, again no difference was noted (Table 3). Thus, 15 of the 22 classical histology cases (68%) had AI of <4 while remaining 32% had AI >4. Similarly, of the 14 desmoplastic variants, 9 (64%) had AI <4 and 36% had AI >4. No difference was observed in the AI : MIB-1 LI ratio between classical and desmoplastic variants (Table 2). This is again obvious on subdividing the tumor groups (Table 3). Thus, of the 22 classical histology cases, 72% (16) had ratio of <0.2 and 28% (6) had ratio >0.2. Similarly, of the 14 desmoplastic cases, 78% (11) had ratio <0.2 and 22% (3) had ratio >0.2. p53 protein was detected immunohistochemically only in 3 of the 90 cases (3.3%). Of these, 2 were of classical histology while 1 was desmoplastic. Bcl-2 protein expression was noted in 7 of all 90 cases studied (7.8%). Three tumors were of classical histology and 4 desmoplastic variants. Follow-up data was available in 40 cases (23 classical and 17 desmoplastic) with a follow-up period from 1 month to 6.5 years (mean 3.5 years). All the 40 cases had undergone suboccipital craniectomy with excision of the tumor. Except for 1 patient, all received postoperative radiotherapy in a dose of 55 Gy to posterior fossa, 25 Gy to spinal cord and 25 Gy to brain. In addition, 34 cases also received chemotherapy. Nineteen patients out of 40 had progressive disease which included 6 cases with residual disease and 13 cases with relapse. In 11 cases, tumor recurred in the posterior fossa while the spinal axis was the site of recurrence in 2 cases only. The 3-year progression-free survival for the whole series of 40 cases was 60% (Figure 7). For those with desmoplastic medulloblastoma, the 3-year progression-free survival rate was slightly better (72%) than for those with classical medulloblastoma (61%). However, the difference did not reach statistical significance (p = 0.561) (Figure 8). Discussion The two main histological variants of medulloblastoma are the "classical" and "desmoplastic" types.1-4 Available literature reports regarding their biology are contradictory. The desmoplastic variant has been reported to occur more frequently among adult patients with a preferential location in one of the cerebellar hemispheres. It was observed in the present study that 70% of classical histology cases occurred in children and 80% were midline in location. In contrast, there was an almost equal distribution of desmoplastic cases in both age groups. Thus, 56% of the total of 43 desmoplastic tumors occurred in children and 44% in adults. Also laterally located tumors were more frequently of desmoplastic histology. The results in the present study are similar to that of Ferrante et al7 who reviewed 1651 patients (1020 children and 631 adult cases) and found that 70-85% of childhood cases were of classical histology and 15-20% were desmoplastic. In contrast, 50-60% of adult cases were classical and 35-40% desmoplastic. In most adult series, the desmoplastic variant is seen in 25-40% cases.5-9 In the study of Giordana et al,10 42 adult medulloblastomas and 42 childhood medulloblastomas were compared and desmoplastic variant was found to be more frequent in adult cases. Histologically, Homer-Wright rosettes representing neuronal differentiation are reported to be more frequent in classical medulloblastomas.4 In contrast, desmoplastic medulloblastomas are especially likely to show astrocytic differentiation.2 The histogenetic significance of the pale islands in desmoplastic medulloblastomas has been studied and cells positive for glial fibrillary acidic protein (GFAP) demonstrated to be associated with these structures.2,11,12 Neuron specific enolase (NSE) has also been shown to be positive in the pale islands, suggestive of neuronal differentiation in these tumors.2,11,24,25 Further confirmation has been obtained on immunohistochemical and ultrastructural studies in which the elongated processes of the cells in the pale islands showed a pattern of co-expression with NSE and tubulin, denoting early neuritogenesis. Thus, pale islands are believed represent progressive patterns of neuronal differentiation along with lesser degree of astroglial differentiation.12 In earlier studies, we have shown using immunohistochemistry and electron microscopy that medulloblastomas have potential for differentiation into glial and neuronal cell lines.26-29 However, no attempt was made in our earlier studies to differentiate between classical and desmoplastic variants. In the present series, we observed astrocytic differentiation both in classical as well as in desmoplastic medulloblastoma (especially in the pale islands). There was no statistically significant difference between the two variants in the percentage of cases showing astrocytic differentiation. In the present series, there was no difference in the MIB-1 LI between classical and desmoplastic medulloblastomas and this is in agreement with the reports of Schiffer et al.21 However, Giordana et al30 reported higher LI in vermian medulloblastomas as compared to hemispheric ones. Also no difference was observed in AI between classical and desmoplastic variants. Schiffer et al21 also described that apoptotic index in both classical and desmoplastic medulloblastomas was the same (1.3+0.5) and did not correlate with proliferation index. The differing survival rates of patients suffering from classical or desmoplastic medulloblastoma were also not reflected in diverging apoptotic indices.22 Schubert and Cervos-Navarro23 observed no correlation of apoptosis to histological variant or evidence of glial / neuronal differentiation. However, they reported higher apoptotic index in male patients corresponding to the reported difference in survival rates between male and female patients. Both proliferation and apoptosis contribute to tumor growth. Hence, both the factors should be taken into consideration while evaluating the net growth rate of a tumor. Again, no difference was noted in the ratio of AI: MIB-1 LI between classical and desmoplastic medulloblastomas. A microfluorometric analysis of DNA content performed by Giangespero et al3 revealed that desmoplastic medulloblastomas represent a homogenous group of neoplasms in terms of histology and DNA distribution. In contrast, classic medulloblastomas are lesions with different degrees of histologically apparent aggressiveness and a complex DNA distribution. However, the studies by Tomita et al31 and Yasue et al32 showed no difference in DNA ploidy between classical and desmoplastic variants. Correlating survival with histological variant in the present study, it was observed that the disease progression-free survival rate at 3 -years for desmoplastic medulloblastoma was slightly higher (72%) than classic ones (61%). However, the difference was not statistically significant. It is generally believed that desmoplastic medulloblastomas have a longer survival.8,18,19 However, contradictory results have been put forward in some large series, mostly pediatric series15,16 and in some adult series17,33 wherein desmoplasia did not seem to affect survival. In a large adult series by Carrie et al,18 desmoplasia was associated with significantly higher survival rate. A clinicopathological analysis of postoperative survival in a large single center group of adult medulloblastoma patients demonstrated a shorter postoperative survival in patients with adequately radiotreated desmoplastic medulloblastoma than in similarly treated patients with non-desmoplastic medulloblastoma.20 In another single institution study, in which desmoplastic lesions were defined on the basis of nodularity, prognosis was significantly better for the patients with classical medulloblastoma.34 The discrepancy in survival may be explained by the fact that in some of these studies, tumors have been classified as desmoplastic on the basis of increased amount of collagen and reticulin fibres with or without the typical nodular pattern of this variant. A more recent study on a series of medulloblastomas with extensive nodularity showed a very favourable outcome despite the fact that majority were poor risk patients and were treated with chemotherapy only.35 Only 3 cases in the present study showed p53 protein expression which is consistent with the results of cytogenetic analysis showing relative paucity of p53 gene mutation in medulloblastomas.36-38 Similarly, Bcl-2 protein positivity was seen only in 7 cases (7.7%) which is in agreement with those of Hara et al.39 The infrequent expression of Bcl-2 which is anti-apoptotic can well be explained in the light of high number of apoptotic cells seen in medulloblastoma. Thus in the present study, the only differences which could be documented between the two histological variants of medulloblastoma were: (i) Age distribution Classical histology cases predominantly occurred in children (70%). Desmoplastic variant showed an almost equal distribution with 56% of the tumors occurring in the children and 44% in adults. (ii) Location Majority (80%) of classical histology tumors were midline in location. Lateral location was seen more frequently with tumors of desmoplastic histology. (iii) Histological characteristics Homer-Wright rosettes were more commonly seen in the classical histology cases. No differences were noted between the two variants with regard to biological parameters of aggressiveness, viz., MIB-1 LI, AI, AI : PI ratio, p53 protein and Bcl-2 protein expression. Also the 3 year progression-free survival did not differ significantly between the variants. Thus, it can be concluded that growth rate (both proliferation and apoptosis) and hence clinical outcome in medulloblastomas does not correlate with histological variant. Acknowledgements Authors wish to thank Mr. Rajeshwar Khadia, Mrs. Kiran Rani, Mr. Anil Bisht and Mr. Gajender Singh for their technical help and Mr. Kamal for secretarial assistance. The work was funded by the Indian Council for Medical Research. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03005f4.jpg] [ni03005f6.jpg] [ni03005f5.jpg] [ni03005f7.jpg] [ni03005t2.jpg] [ni03005f1a.jpg] [ni03005t3.jpg] [ni03005t1.jpg] [ni03005f8.jpg] [ni03005f3.jpg] [ni03005f2.jpg] [ni03005f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}