 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
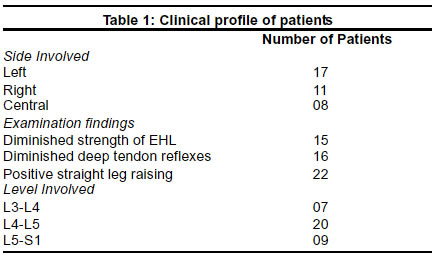
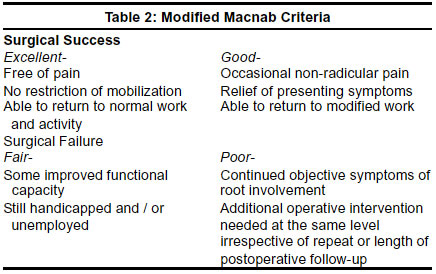
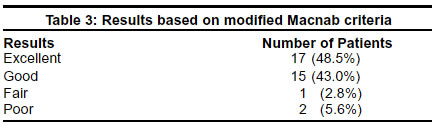
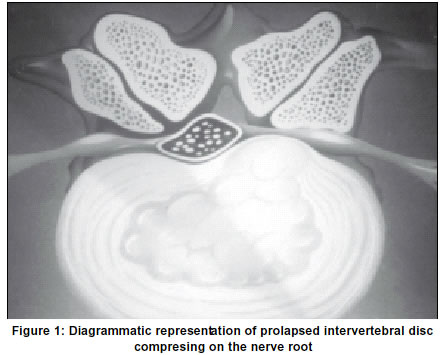
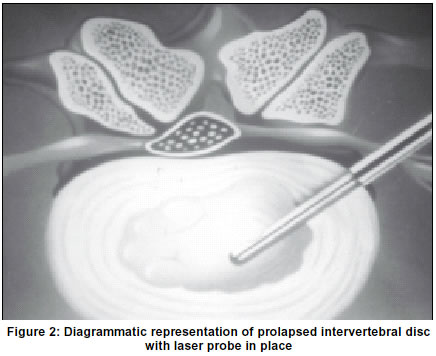
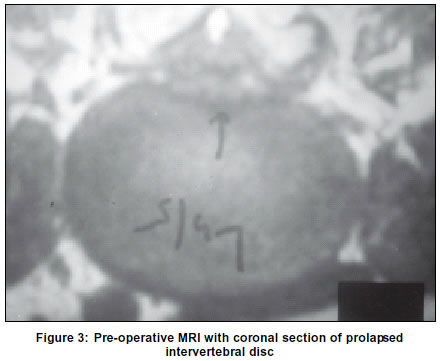
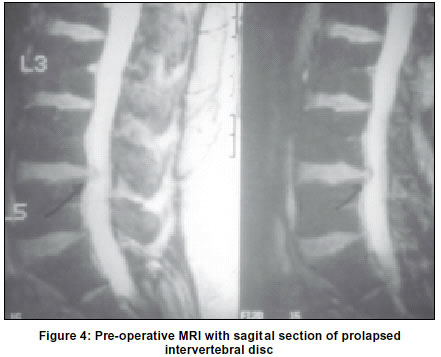
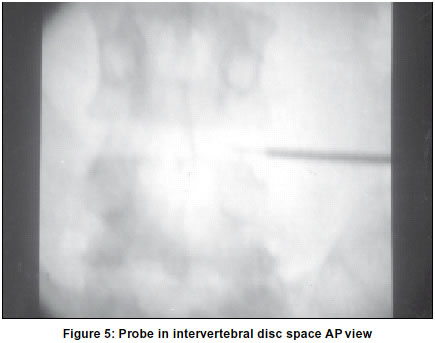
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 35-38 Ho: Yag laser-assisted lumbar disc decompression: A minimally invasive procedure under local anesthesia S. Agarwal, A. S. Bhagwat Department of Orthopedics, P. D Hinduja Hospital and Research Centre, Mahim, Mumbai-400016, India. Accepted on 22.11.2001. Code Number: ni03006 The morbidity associated with open procedures for lumbar intervertebral disc prolapse has led to the development of minimally invasive techniques. Ho: LADD (Laser-assisted disc decompression) is a very cost-effective minimally invasive procedure. The procedure is carried out under local anesthesia The patient can be mobilized immediately after the surgery. The study involved 36 cases treated with Ho: LADD for contained lumbar intervertebral disc prolapse. 35 cases were available for follow-up. There was a 91.5% success rate and a minimal complication rate. All cases adhered to strict inclusion and exclusion criteria and were evaluated with the modified Macnab criteria for the assessment of postoperative results. Key Words: Intervertebral disc prolaps, Laser discectomy. The morbidity associated with open lumbar discectomy has over the period led to microsurgical procedures being devised. Smith in 1964 performed the first percutaneous disc decompression using Chymopapain,9 Schrieber and Suezawa introduced percutaneous endoscopic lumbar discectomy procedures in 1986.8 Choy et al in 1987 introduced laser disc decompression based on the principle that a small change in volume of a contained area results in a large change in the pressure in the same area.2,3 Ho: LADD (Holmium laser-assisted disc decompression) is one of the latest procedures in the array of the various minimal invasive discectomy methods. The following study was carried out to evaluate the efficacy of Ho: LADD done under local anesthesia with a side firing laser probe, in cases of contained lumbar disc herniations. Materials and Methods A total of 195 cases which were operated for lumbar spine affections over a three-year period by a single surgeon, 29 had conventional open procedures, 130 cases had microdiscectomy with or without laminectomy and 36 cases underwent Ho: LADD. The 36 patients who had underwent Ho: LADD were subjected to pre-operative MRI of the lumbar spine, which confirmed a contained intervertebral disc herniation. All patients were assessed and found to adhere strictly to the inclusion criteria (a contained disc confirmed on a MRI, CT, or CT myelogram, a clinical presentation of radicular pain with or without neurological deficits and patients had undergone minimum 6 weeks of conservative treatment). Patients with vertebral and intervertebral stenosis or facet syndrome, previous spinal surgery in the same region, bony deformities such as congenital abnormalities, spondylolisthesis, and hemi-vertebrae, cauda equina syndrome and pregnancy were excluded. All patients were allowed to undergo a minimum of 6 weeks of conservative treatment in the form of bed rest, local heat, analgesics, epidural or oral steroids and physiotherapy. The patient was laid prone on the operating table. The part is prepared and draped under mild sedation with 2mgs of midazolam slow intravenously (IV), supervised by an anesthetist. A prior informed consent was obtained from the patient and the relatives for an open procedure if it was required. The involved level was located with the help of C-arm image intensifier. An entry point was selected 10 cm lateral to the disc space on the symptomatic side. The skin and the tract through which the guide wire is to be passed were infiltrated with 1% Lignocaine. Through a stab incision the guide wire was introduced 8-10 cm at a angle of 35-45 deg. towards the identified disc space. If the patient complained of pain in the leg during the passage of the guide wire, it was promptly removed and reintroduced at a different angle. The wire was kept parallel and midway between the end plates of the symptomatic disc, its position then confirmed on the C-arm. An introducing cannula was passed over the guide wire until it reached the annulus; a trephine was then placed over the guide wire, through the cannula and the position rechecked. The annulus was perforated with the trephine with gentle pressure and rotation through 360 deg.; the trephine and the guide wire were then withdrawn from the cannula. A side firing Holmium laser probe was passed through the cannula and extended 2 cm beyond it. The Holmium laser energy was applied for 5 sec on and off. The intervening time allows the tissues to cool and the gases created by vaporization of the tissues to dissipate. The probe was rotated through 180 deg. so as to create a defect in the disc material. Lasing continued until approximately 1200 joules energy was used within power at 15 watts and repetitive rates at 13 Hertz. The end was achieved when the patient did not complain of radicular pain on increase in the abdominal pressure by pushing against resistance to the foot. At times patients were likely to complain of increased leg pain on the start of lasing due to gas production and subsequent rise in the intradiscal pressure as a result of tissue vaporization. The dissipation of the gases leaves behind a vacuum, which shrinks the surrounding disc material. The wound was dressed and a dose of 500 mg of methyl prednisolone is given postoperatively, oral steroids are then continued in a tapering dose over 10-14 days. The patients are allowed ambulation immediately after the surgery and advised against prolonged sitting and lifting of weights for 4 to 6 weeks. All patients were followed up at 1 week, 3 weeks, 6 weeks, and one year, the average follow-up was of 18 months duration. All patients were rated based on modified Macnab criteria, those with excellent and good were rated as surgical success. Results A total of 36 patients were included in the study, 1 patient was lost to follow-up, and results were obtained in 35 patients. The average age for Ho: LADD was 40 years, for microdiscectomy and open procedures was 41.6 years and 56 years respectively. Of the 36 patients who had radicular pain, 28 patients had predominantly unilateral radicular pain and 8 had bilateral involvement (Table 1) with varying degrees of motor, sensory and autonomic disturbances. There were 24 males and 12 females with the common level of involvement being the L4-L5, followed by the L5-S1 and L3-L4 intervertebral disc respectively (Table 1). The duration of symptoms ranged from 6 to 20 weeks averaging 12 weeks. The commonest level of involvement was L4-5 intervertebral disc. The average hospital stay ranged from 2-4 days, average 3 days. All patients were evaluated according to the modified Macnab rating (Table 2 & 3). Immediate postoperative SLR test was found to be pain-free in all of the operated cases. Of the 15 cases with motor weakness 13 improved and regained full power. The remaining 2 cases were classified as failures and underwent microdiscectomy with subsequent improvement. The recovery of tendon reflexes was not found to be consistent with the overall recovery of the patients. Postoperative back pain that resolved within 48 hours was found to be related to the procedure and responded well to conventional analgesics. Of the three patients categorized as failures, two underwent microdiscectomy for recurrent radicular pain, and had good postoperative relief. The other refused surgery and was treated conservatively. Postoperative complications included severe tingling and numbness on the operated side in a single case, which recovered after 7 day's of oral steroid therapy. Discussion The technique of laser discectomy is relatively new in the whole array of spinal surgery for prolapsed intervertebral disc. Holmium laser discectomy allows for dramatic relief with minimal tissue destruction. Holmium is a rare earth element used along with YAG (Yttrium-Aluminium-Garnet) crystal in the laser to create a photon energy beam as a cold-pulsed energy source. It allows for cutting, coagulation and ablation of the tissues. As compared to Nd: YAG laser which penetrates to a tissue depth of 2 mm, Ho: YAG laser penetrates to only 0.4 mm tissue depth thus preventing extensive damage. Ho: YAG laser is absorbed well in water preventing damage to vital nerve roots and the cord, its short energy burst prevents excessive tissue charring.6 It is important that it not be used in a desiccated disc with low water content. The ablation of the disc material causes a vacuum effect within the disc with shrinkage and in effect relieving pressure from the roots, the so-called implosion theory.1,5 The good results solely depend on proper patient selection and proper needle placement, which are the two most critical influencing factors. The technique has a higher learning curve.7 Difficulties can be encountered with regard to needle placement at L5-S1 intervertebral disc space, especially if the iliac crests ride high making the approach more oblique. Overall success rate of 91.5% in the present study is better than that of W. A. Liebeler at 75% and Sprangfortes and Weirs at 76.9% and 73% respectively.7,10,11 This may be explained by our smaller sample size in comparison and also by the strict selection criteria, which resulted in only 36 cases being selected out of the 195 cases operated in the same period for lumbar spine problems. This series shows a similar trend to that of Choy's study group results, which showed an 84% immediate relief in 182 cases done on an out-patient basis.4 When the cost with regard to hospital stay was compared Ho: YAG LADD proved to be cheaper than open procedures. Though at present it is not possible to carry out this procedure on an out-patient basis due to social and economic reasons, it remains a possibility in the near future. The authors understand the limitations of the present study for the want of a comparative study between the different modalities of treatment. The study also needs to look into the long-term effects of the procedure on the intervertebral disc and the disc space; at present there are no studies which have looked at these two aspects of the procedure. To conclude, Ho: YAG LADD is a very effective, minimally invasive technique with comparable results to other techniques for the treatment of contained intervertebral disc prolapse. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03006t1.jpg] [ni03006t3.jpg] [ni03006f5.jpg] [ni03006f4.jpg] [ni03006f3.jpg] [ni03006t2.jpg] [ni03006f6.jpg] [ni03006f1.jpg] [ni03006f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}