 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 39-42 Endoscopic third ventriculostomy in obstructed hydrocephalus D. Singh, V. Gupta, A. Goyal, H. Singh, S. Sinha, A. K. Singh, S. Kumar Department of Neurosurgery, G. B. Pant Hospital, Delhi, India.
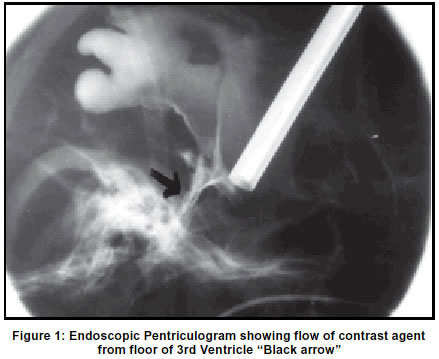
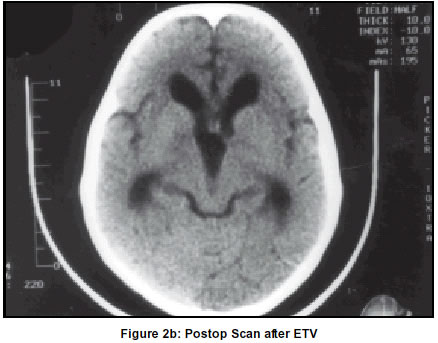
Accepted on 07.12.2001. Code Number: ni03007 Forty-three ETV were performed in 46 patients of obstructive hydrocephalus. Study was divided into two groups. Group 1 was with 29 children of less than two years age. Group 2 had seventeen patients of more than 2 years, adolescent and adults. Group 1 had 70% clinical and 63% radiological improvement whereas Group 2 showed 100% clinical and 73% radiological improvement. ETV failed in relieving the symptoms of hydrocephalus in eight patients. They were eventually benefited with VP Shunt. There was one postoperative death, which was not related to the procedure. ETV is an important alternative to VP Shunt in relieving hydrocephalus due to obstruction in CSF pathway. Key Words: Endoscopy, Hydrocephalus, Third ventriculostomy. The concept of Endoscopic surgery surprisingly started much before the invention of electricity bulb by Thomas Edison (1879). Dandy coined the term `ventriculography' and he is accepted as the father of neuroendoscopy.2 The first successful third ventriculostomy was performed by Mixter.3 Subsequently there have been a number of publications, which have established its role in neurosurgical practice, particularly in hydrocephalus.We present our experience with 46 cases of Endoscopic Third Ventriculostomy (ETV) in obstructive hydrocephalus. Material and Methods Forty-three endoscopic third ventriculostomies (ETV) were performed in 46 cases of congenital obstructed hydrocephalus during the period from Dec.1999 to July 2001. Study population has been subdivided into two Groups [Group 1 - children less than two years of age (29 cases) and Group 2- children more than two years of age, adolescent and adults (17 cases)]. All cases had obstructive hydrocephalus with either features of raised intracranial tension (ICT) or an enlarging head. Enlarged third and lateral ventricles, presence of CSF in subarachnoid spaces and extension of floor of the third ventricle behind and below the dorsum sella were the selection criteria for ETV as suggested by Hoffman.4 ETV were performed under general anesthesia using zero degree Storz operating endoscope. A 1.5 cm skin incision was taken at the level of coronal suture about 3 cm. away from the midline. Lateral angle of the open anterior fontanel was used as an entry point in small children. Burr hole was made with 14 mm burr. The dura was opened and coagulated. Brain surface was coagulated to allow the access of endoscopic sheath (5.6 mm)and trocar into the frontal horn of lateral ventricle. Trocar was removed and zero degree operating endoscope was passed into the sheath. Within the lateral ventricle foramen of Monro was identified using standard landmarks of choroid plexus, thalamostriate and septal veins. Endoscope was then negotiated into the third ventricle whilst protecting the fornices. Fixation of endoscope was done with the Leyla retractor. Once the third ventricle was entered, the mammillary bodies and infundibular recess were identified. Infundibular recess was identified as bright red spot along the anterior limit of the floor of the third ventricle. Floor of the third ventricle was carefully inspected for probable site of the ETV. The site of ostomy was planned at mid- way between mammillary bodies and infundibular recess. Irrigation of ventricle was done with the help of warm ringer lactate at body temperature, particularly in children to avoid hypothermia. Rate of irrigation was kept to 5-8 drops per minute to avoid excessive rise in ICP. Outflow of the endoscope was kept open to allow egress of excessive fluid overload in intracranial cavity. All these procedures were performed after visualization on a monitor with the help of three chip camera. Floor of the third ventricle was punctured with monopolar cautery, Ostomy was enlarged to 6-8 mm size with monopolar coagulaton saving the basilar artery and its branches. Endoscope was then advanced further to look for any second membrane which if present was punctured. Any bleeding from the margin of the ostomy was coagulated. In case of excessive bleeding a constant irrigation and suction clear the fields to a point of coagulation under vision. Once the ostomy was well formed, CSF was seen flowing freely through the opening. To and fro movements of the margins of the ostomy site confirms the patency of the ETV. In case of doubt of patency of the ETV, a 3rd ventriculogram was performed with 3-4 cc of omnipaque injected through the side port of the endoscope. Being more viscous than CSF, efflux of omnipaque through the ostomy site is easily seen on fluoroscopy. A spot X-ray was taken for recording (Figure 1). At this stage the endoscope was slowly withdrawn. Wound was closed in a single layer after coagulating any surface bleeding. Patient was called for follow-up at 15 days, one, two, and six months interval. Results Forty-three ETV were performed in 46 cases. In three cases, ETV could not be successfully performed and a VP shunt procedure was carried out. This was because one patient from Group 1 had unfavorable third ventricular anatomy and two cases in Group 2 had excessive bleeding from the cortical veins. There were 29 children of less than two years age (Group 1) and17 adults/adolescent (Group 2). CT scan was suggestive of aqueductal stenosis in 34 cases and outlet obstruction in 9 cases. There were a number of variations within the ventricular system as seen with the endoscope. A very narrow opening of aqueduct was seen in 22 cases. Imperforated floor of the third ventricle was seen in 8 cases. Postoperative hypothermia was observed in three patients in Group 1, which resulted in delayed recovery from anaesthesia. There was one postoperative death in a 9-month-old child having a poor neurological and physical state prior to surgery. Follow-up period ranged from one to 18 months. Initial clinical improvement was noticed in all cases. However, within one month eight children (Group 1) had recurrent sympotms. CT scan in all these cases showed enlarged ventricles. In three of these cases a repeat endoscopy showed patent ostomy site. VP shunt was done for all these 8 cases. At two months follow-up, clinical improvement was 100% in patients of Group 2 and 70% in patients of Group 1. Radiological regression of the size of the ventricle was seen in 12 patients in Group 1 (63%) and in 11 cases in Group 2 (73%) (Figures 2a & 2b). However, 11 patients,7 in Group 1 and 4 in Group 2 showed significant clinical improvement despite the unchanged size of the ventricle. These eleven patients showed regression in periventricular lucency. There was no case of delayed rise of ICT after 2 months. Discussion Ventriculoperitoneal shunt in the treatment of hydrocephalus is a well-established, safe and a time-tested procedure. However, there are a number of possible problems associated with a shunt procedure.1,5-9 ETV has been used in relieving ventriculomegaly in a number of other clinical conditions such as SAH,8,9 spinal dysraphism,10,11 normal pressure hydrocephalus,12 shunt infections and slit ventricular syndrome8,9 posterior fossa and tectal plate tumours,1,9 and Chiari malformations.9 Obliteration of interpeduncular cistern or tip of basilar artery lying too close to the floor to cause safe perforation are relative contraindications to the procedure. Endoscopic instruments and technique are still evolving. Flexible fibroscope with outer diameter between 2.3 to 4.6 mm13-16 and rigid endoscope with outer diameter between 3.8 to 6.2 mm are more frequently used.1,9,17-20 The current problem is with the fibroscope are its inherent poor image quality, orientation difficulties and inability to fix the scope during the surgery. Rigid endoscope on the other hand is more convenient for third ventriculostomy.17-19,21 A variety of methods have been described for perforating the floor of the third ventricle which include the use of endoscope itself, blunt probe and fogarty catheters,7,14,17 monopolar coagulation19,20,22 and laser fenestration.16,23 Monopolar coagulation helps in perforating the floor and enlarging the stoma. Coagulation produces a peripheral scar around the margin of the ostomy which reduces the risk of restenosis. It is also helpful for simultaneous coagulation of any bleeding point during surgery. The second membrane, the membrane of Liliequist is simultaneously opened with the same instrument. Fixation of the instrument in our series was accomplished with Leyla retractor. The mean time of surgery was reduced from 57 minutes in the first case to 4 minutes in some of the later cases. Following an ETV procedure, the results of a successful surgery are seen in terms of clinical and radiological improvement. The clinical improvement in aqueductal stenosis following ETV is variable. It ranges from 56% to 87%.19,24,25 Adults have a better outcome than children.1 Most authors feel that the outcome is better in children of more than 2 years of age.22,26-29 In those younger than 2 years, the clinical improvement is less than 50%. Some have reported 100% failures in less than one year of age with aqueductal stenosis while others have found no correlation with age.9 In our series clinical improvement was 100% in Group 2 whereas Group 1 had 70% clinical recovery. Poor results among children in Group 1 could be due to poor development of CSF absorptive surfaces. Unfortunately, a non-invasive test is currently not available to predict the response to internal shunting such as ETV. Even invasive infusion test may not be reliable. Stoma closure has been reported in 8% resulting from restenosis, particularly in those patients with high CSF protein and fibrinogen levels or in patients with some intraoperative bleeding.1 It has been observed, particularly in cases with chronic hydrocephalus, that the clinical improvement occurs even without changes in the size of the ventricle. Radiological improvement after ETV varies from 53-87%.1,25,30,31,37 In our series overall radiological improvement was 63% and 73% in patients of Group 1 and Group 2 respectively. It is also well documented that radiological improvement in the form of regression of size of the ventricle or decrease in periventicular lucency/ edema takes a longer time than clinical recovery. MR flow studies,32,33 ultrasound33 can confirm the patency of the ETV. Third ventriculography also provides similar informations. Technical failures of endoscopic procedures vary from 5-26%.1,6,9 The most common cause of failure is bleeding from cortical veins or intraventricular bleed. Early failure within one month is either due to poor absorptive surface or poor procedure. Late failures are due to stoma closure.1,2,9 A major bleed from the basilar artery or its branches can be fatal.34,35 Intraoperative Doppler can be a useful tool to avoid injury to major vessels.36 Hypothermia is a common observation due to cold irrigating fluid. Injury to fornices, hypothalamus, thalamus, 3rd nerve, are possible.37,38 Endoscopic third ventriculostomy is rapidly becoming popular as a new method for treatment of hydrocephalus. There are a number of advantages of ETV over VP shunt in the treatment of hydrocephalus. There are no shunt related problems. Further there are no low pressure complications as seen with VP shunt. It can also be performed in those who are previously shunted and has resulted in shunt independent life in 76% cases.24 Being a short procedure, patient anesthesia and operation time is significantly reduced. Hospital stay is short and overall it is much more economical than a VP shunt. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03007f2b.jpg] [ni03007f1.jpg] [ni03007f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}