 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
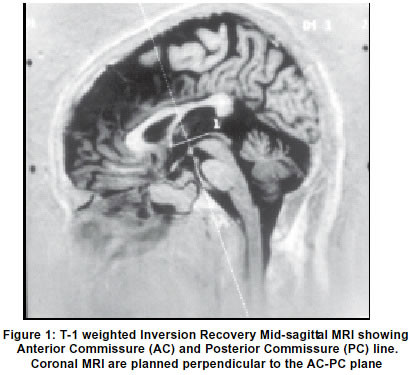
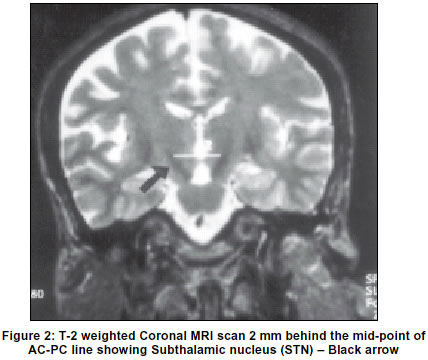
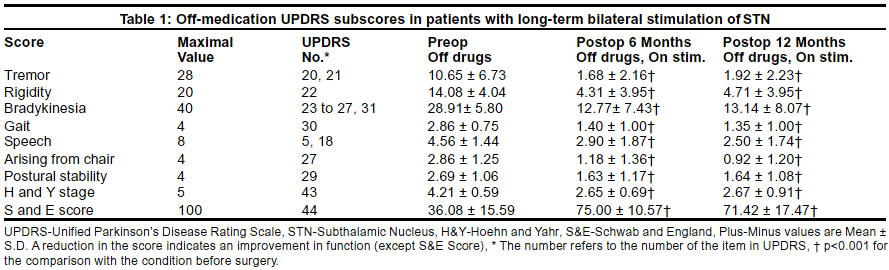
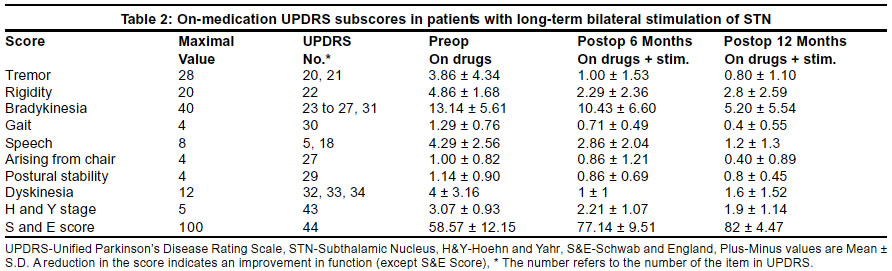
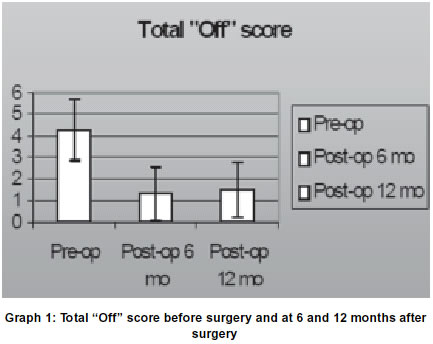
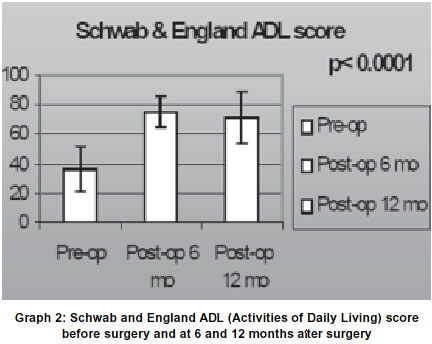
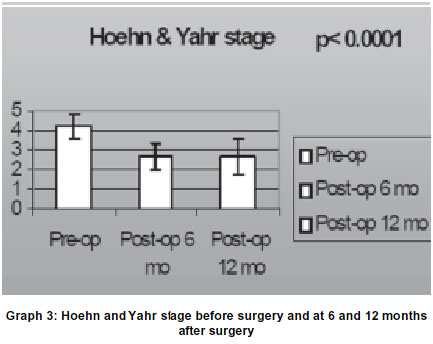
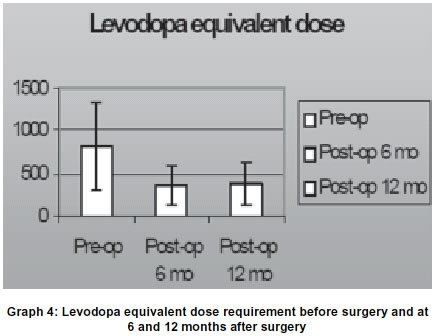
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 43-48 Bilateral subthalamic nucleus stimulation for Parkinson's disease P. K. Doshi, N. A. Chhaya, M. H. Bhatt Jaslok Hospital and Research Centre, Mumbai, India. Accepted on 21.12 2001. Code Number: ni03008 High frequency stimulation of the subthalamic nucleus (STN) is known to ameliorate the signs and symptoms of advanced Parkinson's disease. Aim: We studied the effect of high frequency STN stimulation in 23 patients. Method: Twenty-three patients suffering from severe Parkinson's disease (Stages III-V on Hoehn and Yahr scale) and, particularly bradykinesia, rigidity, and levodopa-induced dyskinesias underwent bilateral implantation of electrodes in the STN. Preoperative and postoperative assessments of these patients at 1, 3, 6 and 12 months follow-up, in "on" and "off" drug conditions, was carried out using Unified Parkinson's Disease Rating Scale, Hoehn and Yahr staging, England activities of daily living score and video recordings. Results: After one year of electrical stimulation of the STN, the patients' scores for activities of daily living and motor examination scores (Unified Parkinson's Disease Rating Scale parts II and III) off medication improved by 62% and 61% respectively (p<0.0005). The subscores for the akinesia, rigidity, tremor and gait also improved. (p<0.0005). The average levodopa dose decreased from 813 mg to 359 mg. The cognitive functions remained unchanged. Two patients developed device-related complications and two patients experienced abnormal weight gain. Conclusion: Bilateral subthalamic nucleus stimulation is an effective treatment for advanced Parkinson's disease. It reduces the severity of "off" phase symptoms, improves the axial symptoms and reduces levodopa requirements. The reduction in the levodopa dose is useful in controlling drug-induced dyskinesias. Key Words: Subthalamic nucleus, Parkinson's disease, deep brain stimulation, Dyskinesia. Parkinson's disease (PD) is a common movement disorder characterized by rigidity, bradykinesia, tremor and postural instability. Replacement of deficient dopamine is effective in relieving these symptoms and this has been used to clinically confirm the diagnosis of PD in the absence of a laboratory test. This `honeymoon' period continues for 7 to 10 years when most symptoms of PD can be suppressed and patients live almost normal lives albeit with dopamine replacement. Later motor complications make their appearance. Wearing off phenomena, peak-dose dyskinesia, biphasic dyskinesia, "off" phase dystonia need different medical strategy such as the use of Dopamine Receptor Agonist (DRA). Once medical options are exhausted, surgery is a good and viable option. The reason for surgery as an emerging and viable option is based on better understanding of the basal ganglia circuitry and the pivotal role of subthalamic nucleus (STN) in producing signs and symptoms of PD. Increased activity of the STN is a well-established characteristic of a parkinsonian state1-4 and this excitatory output onto the globus pallidum pars interna (Gpi) and substantia nigra reticulata (SNr) produces motor signs in the MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) monkey model of PD.5-7 High frequency stimulation of the STN, leading to continuous depolarization in turn inhibiting the STN, has shown to ameliorate symptoms of Parkinson's disease.8-11 We present our experience of deep brain stimulation (DBS) of STN in twenty-three cases. Material and Methods Twenty-three patients (18 men and 5 women) with a mean (± SD) age of 58 ± 9.3 at the time of surgery, with advanced PD, were selected to undergo bilateral STN stimulation. The selection criteria included confirmed diagnosis of PD12 by a neurologist specialized in Movement Disorders, excellent response to levodopa and absence of any cognitive deficits (score³ 24 on Mini-Mental test).13 All the patients suffered from motor fluctuations, "off" phase dystonia, dyskinesias or gait disorder inadequately controlled by the available pharmacological means. Well-motivated patients able to carry out reasonable amount of activities of daily living (ADL), when in an "on" phase, were selected for surgery. Patients with other serious medical or surgical conditions were excluded. Despite the above strict selection criteria one patient with advanced but stable peripheral neuropathy was operated upon, as his Parkinson's disease needed urgent attention. Five patients had undergone previous unilateral pallidotomy. The pre-selected patients were admitted two days prior to surgery for pre-surgical evaluation and fitness to undergo this surgery. Parkinsonian disability was scored using standard rating scales_Unified Parkinson's Disease Rating Scale (UPDRS), Hoehn & Yahr (H&Y), Schwab and England (S&E).14 This was done during best "on" and 12 hours "off" medication condition. Video recordings were also carried out twice. Cognitive assessment was performed using Mini-Mental test. Postoperative assessment was done at 1,3,6 and 12-month intervals. This was performed in two stages - First in "on" medication and "on" STN stimulation, second in "off" medication and "on" STN stimulation. The surgery was performed using CRW (Cosman-Robert Wales) stereotactic system. The anatomical target localization was performed using computerized tomography (CT) and magnetic resonance imaging (MRI). An inversion recovery, sagittal MRI was obtained to identify the anterior commissure (AC) and posterior commissure (PC) (Figure 1). A heavily T2 weighted coronal MRI sequence was then obtained perpendicular to the AC-PC plane. The STN was typically identified on a slice 2 mm posterior to the mid-commissural point (Figure 2). Usually, this also correlated with the anterior margin of the red nucleus.15 STN target was identified 2 mm posterior to the mid-commissural point and 11-12 mm lateral and 4 mm inferior to this plane. Axial computerized tomography (CT) scan was performed to double-check the MRI coordinates. Once the anatomical target was calculated, the stimulating electrode was inserted through a pre-coronal burr hole. Motor stimulation was performed at 5 Hz frequency and the sensory stimulation was performed at 100 Hz frequency. Stimulating electrodes were used to stimulate the STN and gauge the patient's response to both motor and sensory stimulation. The neurologist (MHB) present in the operation theater assessed the improvement in tremors, rigidity and bradykinesia. Once the confirmation of the STN target was obtained, the stimulating electrode was replaced with DBS electrode (Medtronic DBS electrode 3389-40). The final position was confirmed at optimal improvement in rigidity and bradykinesia without any motor side effects. Presence of dyskinesia on the table during sensory stimulation was considered to be a positive confirmatory sign for target localization. Both the electrodes were implanted on the same day. The next day, under general anesthesia, the pulse generator (Itrel 2 or Kinetra) was implanted in the infraclavicular fossa. [This programmable battery also known as IPG (Implantable Pulse Generator) provides current at desirable rate and voltage]. Postoperative CT scan was performed to confirm the position of the electrodes. Monopolar programming was adopted with one of the contact points in the STN being negative and the Implantable Pulse Generator (IPG) being positive. To start with, each contact was assessed for improvement in parkinsonian disability. The best contact with low threshold for improvement and high threshold for side effects was selected for final continuous stimulation. Programming was started with pulse width of 60 msec and frequency of 130 Hz from the second postoperative day. Drug reduction was commenced on day 3 or 4 postoperatively. Preoperatively, patients were on mean (± SD) levodopa equivalent dose of 813.63± 513.83 mg. In order to assess changes in medication for the entire group, preoperative and postoperative total levodopa equivalent doses were calculated. Equivalents of 100 mg of levodopa were 133 mg of sustained release levodopa, 10 mg bromocriptine or 1 mg pergolide. All the patients were on at least one dopa agonist preoperatively. Amantadine and Pacitane doses were not reflected in the dose analysis. The primary outcome measures were the scores on part II (activities of daily living) and part III (Motor examination) of the UPDRS. The secondary outcome measures were the subscores of UPDRS part III, which evaluates akinesia, rigidity, tremor, gait, postural stability and dyskinesias; S&E scores for global activities of daily living and H&Yscores.16 The data was analyzed using Student's t-test. Results Fourteen patients were followed up for one year and twenty-three patients for six months. Bilateral STN stimulation significantly reduced the motor score (part III of the UPDRS) in "off" medication phase in all the patients, at six months by 53% and at one year by 61% (p<0.0005). The reduction in the motor score in the "on" medication "on" stimulation phases at 6 months was 30% and at 12 months was 33%. The improvement in the part II of UPDRS, which reflects the activities of daily living, in the "off" medication "on" STN stimulation situation was 43% at 6 months and 62% at 12 months (p<0.0005). The improvement in ADL in the "on" stimulation "on" medication situation was 36% at 6 months and 53% at 12 months. Long-term stimulation resulted in improved scores for bradykinesia, rigidity, tremor, gait, postural stability and impairment in arising from chair, when patients were evaluated "off" medication (Table 1). When evaluated in "on" medication "on" stimulation condition the scores did not show statistically significant improvement (Table 2). The duration of the "off" phase was reduced from 2.36 ± 0.74 to 0.71 ± 0.61 (p<0.001) (Graph 1). The intensity of symptoms was mild during this phase and 7 patients did not experience any "off" state. The improvement that was seen in patients at 6 months persisted at 12 months follow-up. Pain and "off" phase dystonia were present in 11 patients preoperatively, this resolved in 10 patients and in one patient the severity had decreased. As a result of clinical improvement, the scores of the S&E ADL also improved from 36.08 ± 15.59 preoperatively to 75 ± 10.57 and 71.42 ± 17.47 postoperatively at 6 and 12 months follow-up, in "off" medication phase (Graph 2). The scores compared during "on" medication phase did not improve to a statistical significance. The H&Y scores in "off" medication phase improved from 4.21 ± 0.59 preoperatively to 2.65 ± 0.69 at 6 months and 2.67 ± 0.91 at 12 months postoperatively (Graph 3). The change in the scores in the "on" phase was negligible. Twenty-two patients suffered from dyskinesias preoperatively. The preoperative dyskinesia score was 4.69 ± 2.47 and postoperative dyskinesia score was 1.12 ±1.64 at 6 months and 1.9 ± 2.23 at 12 months. A reduction in the levodopa equivalent dose was achieved in all the patients. Two patients went off medication after surgery. One patient continued only on dopa agonists. The mean levodopa dose was reduced from 813.63 ± 513.83 preoperatively to 359.09 ± 220.73 at 6 months and 378.57 ± 245.50 at 12 months (Graph 4). The average current parameters were 60 msec of pulse width and 130 Hz frequency, with the average voltage of 2.42± 0.78. Postoperative programming was started from the second postoperative day to assist reduction in hospital stay. The programming was performed as per the standard guidelines.17 The programming contact was selected based on the information obtained from the postoperative CT scan, operative notes and clinical response to the varying voltage. Programming session was scheduled once a day. The patient and the caretaker were advised to keep the diary of various "on", "off" and dyskinetic states. The programming and drug adjustments were performed simultaneously to get a smooth control of PD. Eighteen of the twenty-three patients were discharged with a stable current setting. Five patients required weekly follow-ups for further adjustments of the stimulator settings. None of the electrode contacts had to be changed during follow-up evaluations once the patient had been stabilized. Two patients were readmitted for reprogramming after discharge. These patients lost their initial benefit of programming and deteriorated in their clinical condition during follow-up. Both these patients had less than satisfactory response at the time of discharge. Their symptoms improved following change of contacts and reprogramming. Two patients developed device-related complications. One diabetic patient developed doubtful infection at the scalp connector site. He was hospitalized immediately and successfully treated with intravenous antibiotics. Another patient, who was very lean, injured himself over the IPG and developed breach in the skin exposing the IPG. The IPG was explanted and he was treated with intravenous antibiotics. The IPG was implanted on the right side after healing of the left side wound. Two patients had abnormal weight gain. Their food habits had changed and they put on 2 kg of weight within a week after surgery. At the time of follow-up they had gained 10 kg and 12 kg weight. One 75-years-old patient developed deterioration in gait, nine months following surgery. He was hypertensive, and on clinical examination he had bilateral extensor plantar response. His MRI was difficult to interpret due to artifacts from the electrodes, but did not reveal any major infarct, there was however, generalized cortical atrophy, more marked in the frontal region. One patient developed dystonic posturing of the upper limb six months following surgery, which initially responded for few hours, to reintroduction of levodopa (he had been taken off all medication following surgery). This benefit was temporary and at the last follow-up (18 months), the dystonia is worsening and involving the other upper limb also, despite levodopa and adjustments of stimulation parameters. Discussion We found that bilateral STN stimulation significantly improves "off" state in patients with severe PD as reflected by change in bradykinesia, rigidity, tremors and gait. This improvement was also reflected in activities of daily living and reduction in the "off" period. Six patients who had been off work for 3-5 years prior to surgery could resume their work. All the patients had become independent in their activities of daily living. The improvement was equally marked in appendicular (bradykinesia, rigidity and tremor) and axial symptoms (gait, posture, balance and standing up from sitting position). The "on" periods were more predictable, of longer duration and smooth. The unpredictable and sudden "off" episodes that these patients used to experience prior to the surgery were abolished. The "off" period symptoms were mild and patients were able to carry out their activities in "off" phase also. These findings are in confirmation with those published by others.18-20 There was improvement in the postoperative "on" medication "on" stimulation phase as compared to the preoperative "on" medication state, but this did not reach statistical significance. Five patients had undergone unilateral pallidotomy prior to STN stimulation. They were offered bilateral STN stimulation, as it is known that bilateral pallidotomy has adverse effects on speech and cognition.21-23 These patients had "off" phase dystonia and pain on the ipsilateral side of pallidotomy. In two patients it persisted on the contralateral side also, despite pallidotomy. STN stimulation alleviated the dyskinesias, dystonia and associated pain in all these patients. These patients required more careful programming and finer drug adjustments to achieve good outcome. Levodopa-induced dyskinesias are a major problem of advanced Parkinson's disease. Following bilateral STN stimulation, there is an initial transient worsening of the dyskinesias.24-26 However, the beneficial effects of the stimulation allow concurrent reduction in the Levodopa dose and this in turn helps in eliminating the dyskinesias. We were able to control dyskinesias in all patients except one. In this patient, who had a previous pallidotomy, the dyskinesias were induced by a very small dose of levodopa on the side ipsilateral to pallidotomy. Gradual drug reductions and frequent current adjustments made it possible for us to stabilize him over four months time. Patients with advanced Parkinson's disease are known to suffer from marked axial symptoms. These axial symptoms, in the form of gait disturbances like retropulsion and propulsion, difficulty in getting in and out of bed and arising from chair and postural instability, are not possible to improve upon even by the best medical adjustments at this stage. Bilateral STN stimulation is perhaps the only surgical modality so far available, which has marked improvement in these axial symptoms. The axial symptoms are known to improve in the "on" and "off" phase. The improvement in axial symptoms has also been known to sustain over a period of time. Conclusion Bilateral STN stimulation has been found to be an effective surgical therapy for treating advanced PD. It has been able to improve the most disabling axial symptoms of gait and postural instability that fail to respond to other modes of therapy. The effect of STN stimulation is constant over time without the patient developing any significant tolerance to stimulation current. The side effects induced by current settle down after some time. Special attention must be paid to patient selection. We also suggest conveying a word of caution to patients and relatives regarding the efficacy of surgery, to avoid unrealistic expectations. Acknowledgements The authors are thankful to Research Society of Jaslok Hospital and Research Centre for funding this project, to Dr. Joy Desai for assisting in edition of manuscript, to Dr. Ujwal Bhure for statistical analysis and to Mr. Kamal Kapoor for helping in preparing manuscript. We are also thankful to Dr. N. H. Wadia and Dr. S. M. Katrak for allowing us to use their case material for preparing this manuscript. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03008g2.jpg] [ni03008g1.jpg] [ni03008f1.jpg] [ni03008f2.jpg] [ni03008g3.jpg] [ni03008t2.jpg] [ni03008t1.jpg] [ni03008g4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}