 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 49-51 Morbidity predictors in ischemic stroke J. N. Panicker, M. Thomas, K. Pavithran, D. Nair, P. S. Sarma Department of Hematology, Medical College, Thiruvananthapuram, Kerala-695011,
India, and Department of Neurology, Achutha Menon Centre for Health Science
Studies, Sree Chitra Thirunal Institute for Medical Sciences and Technology,
Thiruvananthapuram,
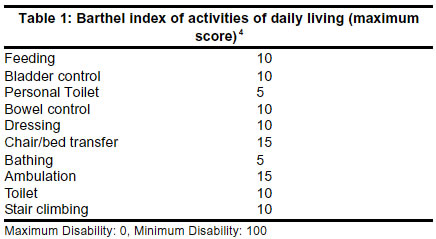
Kerala695011, India. Accepted on 01.01.2002. Code Number: ni03009 Background: Although ischemic CVA is one of the leading causes for death and disability, parameters for predicting long-term outcome in such patients have not been clearly delineated, especially in the Indian context. Methods: A prospective hospital-based study of 105 patients of ischemic stroke, focal neurological deficits and functional score was assessed and the C-reactive protein level (CRP) was measured. A follow-up was done at 5 days and at 6 months and outcome variable was the functional status at 6 months using Barthel Index of Activities of Daily Living. Accordingly, patients were grouped into 3 - Barthel Index < 41: Severely disabled, Barthel Index 41-60: Moderately disabled and Barthel Index > 60: Mildly disabled. Results: At admission, if upper limb power was less than Medical Research Council (MRC) grade 4, or aphasia was present or CRP assay was positive, then at 6 months, these patients most likely belonged to the severely disabled group. If upper limb or lower limb power was greater than MRC grade 3 or there was no aphasia or conjugate gaze deviation or CRP assay was negative, these patients most likely belonged to the mildly disabled group at 6 months. Follow-up rate was 86%. Conclusion: Patients can be stratified according to the predicted prognosis. The treatment and rehabilitation can be properly planned and strictly adhered to in patients predicted to have worse prognosis. Key Words: Acute-phase reaction, Arteriosclerosis, Barthel Index, Cerebrovascular disorders, C-reactive protein, Inflammation, Stroke, Ischemic. Stroke (cerebrovascular accident- CVA) is defined as rapidly developing clinical signs of focal (at times global) disturbance of cerebral functions, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.1 With an annual incidence of 0.2 to 2.5 per 1000 population, CVA is an important health problem worldwide.2 In India, annual incidence of stroke is 33 per 100,000 and mortality rate 73 per 100,000.3 Though ischemic CVA is one of the leading causes for death and disability, parameters for predicting long-term outcome in such patients have not been clearly delineated, especially in the Indian context. The prognostic factors studied should be simple, conclusive and assessable at all levels of the health care system. With this background, this prospective study was planned and executed. Materials and Methods One hundred and five patients of CVA admitted in the medicine wards of Medical College Hospital, Thiruvananthapuram from 1st September 1999 to 31st December 1999 were chosen for this longitudinal study. Inclusion criterion was acute onset of focal neurological deficits with CT scan excluding hemorrhage and stroke mimickers such as intracranial infections, subdural hematoma or tumor. Patients with any clinical evidence of infection or inflammation were excluded. Outcome variable was functional status at 6 months using the Barthel Index of Activities of Daily Living (Table 1). Each patient was assessed according to a fixed protocol. The first evaluation was conducted 24-48 hours after admission. A detailed clinical profile was obtained. Neurological deficits such as aphasia, cranial nerve palsies, limb weakness, sensory impairment, cerebellar dysfunction, conjugate gaze deviation and hemianopia were elicited by a standard comprehensive bedside neurological examination. Functional score was assessed using Barthel Index. C-reactive protein (CRP) was measured by semi-quantitative assay using latex agglutination slide test (Tulip Diagnostics). Patients were reassessed on the 5th day and condition reviewed. Proper nursing care and physiotherapy were explained to the relatives, caregivers and whenever possible, to the patient. Third evaluation was at the 6th month of follow-up and involved either telephone or postal correspondence with a reliable informant. Improvement was objectively assessed by determining the functional status using Barthel Index. Doubts and apprehensions of the relatives, caregivers and patients were addressed and cleared. Importance of nursing care and physiotherapy were re-emphasized and a sense of confidence and hope were instilled. According to the Barthel Index, patients were divided into 3 groups:5 Barthel Index < 41: Severely disabled
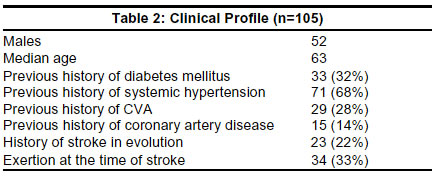
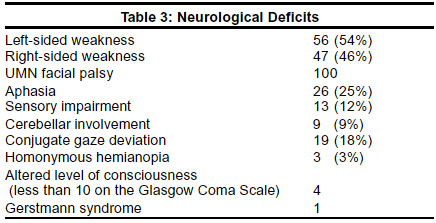
Detailed analysis of data was performed and SPSS for Windows version 6 was used for statistical analysis. Univariate analysis was done by Chi square test and multivariate analysis by logistic regression. Results Table 2 shows the clinical profile of 105 patients. Most patients developed stroke in the morning hours, 6 a.m. to 2 p.m. Table 3 shows the neurological deficits. C-reactive protein measurement was done in 92 patients and was positive in 50 (54%). While 26 patients had a CRP level of 0.6 mg/dL, 24 had a value of 1.2 mg/dL. Except for 3 patients, all patients with aphasia had positive CRP and except for 2 patients, all patients with conjugate gaze deviation had positive CRP. 12 patients had normal CT study while 18 had multiple infarcts. The most commonly affected was the middle cerebral artery and the lentiform nucleus was the commonest site for infarction. Follow-up at 6 months was 86%. Fifteen patients were lost to follow-up and 17 expired. Barthel Index at day 1 was found to correlate with that at 6 months, correlation coefficient 0.64. Following statistical analysis, it was found that at admission, if the upper limb power is less than Medical Research Council (MRC) grade 4, or aphasia is present or CRP assay is positive, then at 6 months, these patients most likely belonged to the severely disabled group. If at admission, the upper limb or lower limb power was greater than MRC grade 3 or there is no aphasia or conjugate gaze deviation or the CRP assay is negative, then at 6 months, these patients most likely belonged to the mildly disabled group (p<0.01). Discussion The present work is a longitudinal hospital-based study focusing on the prognostic factors following ischemic CVA and includes follow-up at 6 months. Hemorrhagic stroke was not included to maintain homogeneity in the sample population. Patients with clinical evidence of systemic infection or inflammation were dropped to exclude the other causes for elevated CRP. The inclusion and exclusion criteria as well as duration of follow-up were chosen based on similar studies done from other centers in the world.6 Follow-up was achieved through telephone in most of the cases and postal correspondence only in those without access to telephone. Activities of daily living reported by telephone interviews have been shown to correlate highly with those measured from direct examination. This novel method ensured a good follow-up of 86%. By directly communicating over telephone, a close rapport could be maintained. Even without coming to Medical College Hospital, patients, relatives and caregivers could clarify doubts arising after discharge from the hospital. Those patients with complications during the follow-up period were advised to attend the out-patient department for further evaluation. Significant changes in the disability pattern were not expected during the immediate post-stroke period. Hence 6 months was chosen as the follow-up period. By 6 months, maximum functions would have been regained and the long-term functional disabilities could be studied accurately. That CRP elevation has a bearing on the functional disability at 6 months is an important finding in this study. C-reactive protein is the prototype of the acute phase proteins as it shows earliest and maximum elevation in inflammation.7 It is secreted by the liver in response to a variety of inflammatory cytokines and levels rise following trauma, inflammation and infection.8 While CRP is a well-known prognostic factor following coronary events,9 association with CVA is not well delineated. C-reactive protein may be elevated following ischemic stroke because of inflammation consequent to cerebral infarction, inflammation consequent to the unstable atherosclerotic plaque and complications secondary to stroke.6 Latex agglutination was used for estimating CRP levels as it is easily available, simple and cost-effective as compared to nephelometry, which had been employed by Muir et al.6 Normal value is below 2 mg/L.10 Thus prognosis following ischemic stroke can be determined without much burden on the existing infrastructure of the health care system. Serial measurement of CRP was not within the scope of this study, but may be planned in future studies, especially if a newer treatment modality focusing on plaque inflammation is to be studied. The present study did not include factors that could modify the end point such as compliance to treatment and occurrence of co-morbidities. But this has not been taken into consideration in previous studies such as Muir et al6 and hence the results are comparable. Upper limb power was found to be an important prognostic factor. This was despite the fact that Barthel index involves tasks of both upper and lower limbs (Table 1). Prescott et al also derived a similar conclusion.11 Significance of aphasia can be on two counts. Firstly, it implies a larger area of infarction. Secondly, as 14 of the 26 patients were having global aphasia, rehabilitation and performance of activities as per Barthel index would have been difficult. However, some studies have indicated that there is no association between aphasia and prognosis.12,13 This is due to differences in the scale used to assess functional status. A larger sample size would be required to evaluate the importance of the observation. While the univariate analysis showed that several of the predictor variables had a statistically significant association with the outcome variable, only upper limb power was found to be significant after adjusting for other variables by multivariate analysis. This can be attributed to the small sample size. The findings of this study are significant for several reasons. C-reactive protein level at admission was found to be a predictor of functional disability in ischemic CVA. Unlike in the previous study by Muir et al6 where end point taken was mortality, the present study has studied morbidity (functional status) and hence has gone one step forward. A detailed literature search revealed that it may be the first time that morbidity predictors of ischemic CVA have been studied in the Indian context. The follow-up generated an enthusiastic response of 86%. The relatives, caregivers and patients were immensely benefited. Cerebrovascular accident is an important health problem and is one of the leading causes for morbidity and mortality. The variables found in this study can be used to predict prognosis even at the peripheral hospitals. This helps in stratification of patients depending on the likely outcome and will help the treating physician and the relatives. Though intensive and scientific physiotherapy and rehabilitation can be planned for all patients with ischemic CVA, the protocol is to be strictly adhered to in patients predicted to have worse prognosis so that they receive maximum support and assistance. Prognosis can be discussed with caregivers and relatives and the social implications of the illness can be addressed even before the patient is sent home. The relationship between CRP and cerebrovascular diseases has a bearing on newer treatment modalities of the future. As a subset of patients with stroke has elevated CRP, the role of anti-inflammatory agents and antibiotics in the acute management of such patients is to be addressed. As elevated CRP is an index of increased risk for cardiovascular disease, these patients can be targeted with more aggressive conventional therapy, or new therapies, for plaque stabilization. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03009t3.jpg] [ni03009t2.jpg] [ni03009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}