 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
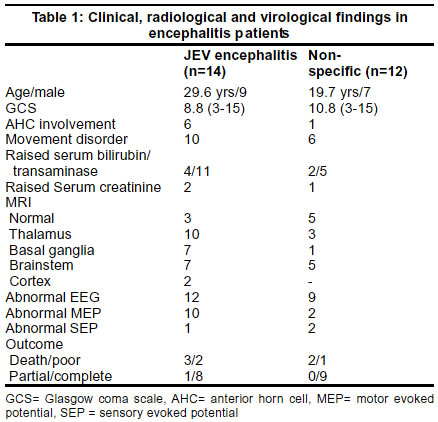
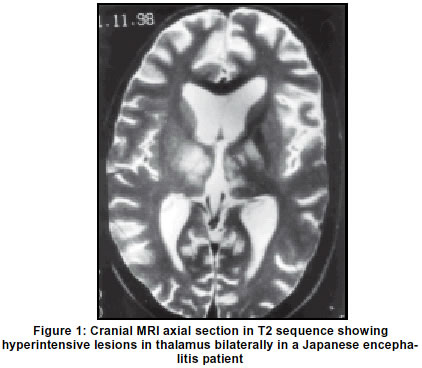
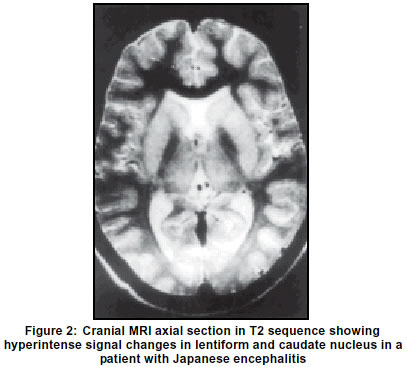
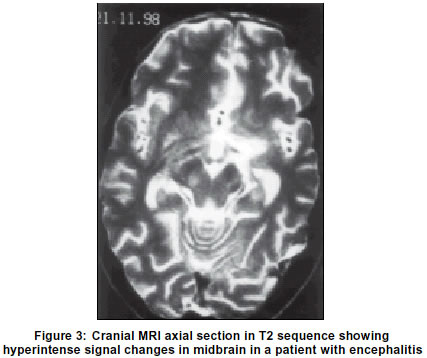
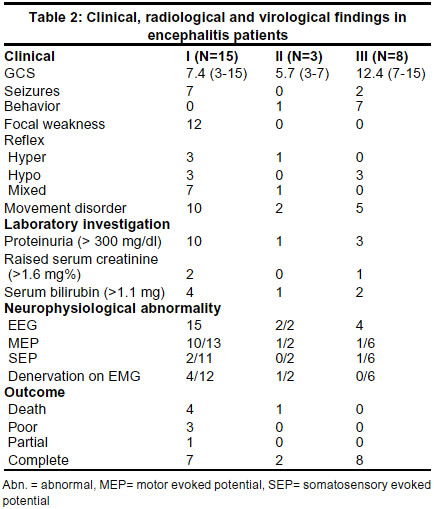
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 55-59 Clinical, radiological and neurophysiological spectrum of JEV encephalitis and other non-specific encephalitis during post-monsoon period in India U. K. Misra, J. Kalita, D. Goel, A. Mathur* Department of Neurology, Sanjay Gandhi PGIMS, Lucknow, India, and *Department of Virology, KG Medical College, Lucknow, India. Accepted on 31.01.2002. Code Number: ni03011 Aims: To study the spectrum of encephalitis during the post-monsoon period in a tertiary care centre of India. Methods: Clinical, neurophysiological and radiological features of patients with encephalitis are reported in this communication. The patients were subjected to clinical examination, CT or MRI scan, EEG, motor and somatosensory evoked potentials in both upper and lower limbs bilaterally and concentric needle electromyography. The laboratory studies for Japanese encephalitis (JE) comprised virus isolated, IgM capture ELISA, mercaptoethanol test and hemagglutination inhibition titre in paired sera against JE virus. Patients were classified into JEV encephalitis and non-specific encephalitis. On the basis of radiological features, they were classified into group I (thalamic or basal ganglia involvement), group II (brainstem involvement only) and group III (normal MRI). The outcome was defined into poor (bedridden), partial (dependent for daily activities) and complete (independent) recovery at the end of 3 months. Results: Out of 26 patients (Age 7-70 years, mean 24.8 years), laboratory evidences of JEV infection was present in 14 patients and one patient had herpes simplex encephalitis. The patients with JEV encephalitis had more severe illness as evidenced by lower GCS score, higher frequency of anterior horn cell involvement, movement disorders and more extensive MRI changes. The EEG and MEP changes were also more frequently abnormal in the JEV group. On radiology, 15 patients had thalamic or basal ganglia involvement (group I), 3 isolated midbrain involvement (group II) and 8 had normal MRI (group III). Laboratory evidence consistent with JE were present in 11 out of 12 patients in group I and 3 out of 8 in group III, however, there was no laboratory evidence of JE virus infection in patients with isolated brainstem involvement. There was overlap in the neurologic and systemic manifestations in all the 3 radiological groups as well as in the groups with and without laboratory evidences of JEV infection. Conclusion: The observed overlap in neurological and systemic involvement in different subgroups of encephalitis may be due to JE or JE-like viral infection. The possibility of strain variation, change in virulence of organism or immunity of host needs further studies. Key Words: Encephalitis, Japanese, Imaging, Electroencephalography. Viral encephalitides are common in developing countries including the Indian subcontinent. The common viruses producing encephalitis are Japanese encephalitis virus (JEV), dengue, Westnile, mumps, measles, polio, coxasackie, echo, enterovirus 70, rabies and Kyasanur forest disease. Japanese encephalitis (JE) is the commonest human endemic encephalitis in the world. About 50% cases of JE occur annually in Asia.1 The mortality of JE ranges between 20 to 40%.2,3 JE is a disease of rural areas closely linked to paddy cultivation, pig farming and mosquito breeding in water-filled paddy fields. Because of poor infrastructure in rural areas, the cases of JE are poorly investigated with modern investigative techniques. In a tertiary care hospital, we have been seeing 10-15 patients with encephalitis in the post-monsoon period (May to November) and the majority of these were JE; occasionally due to measles, mumps, herpes simplex and polio. In the year 1998, because of unusually heavy rains and flood, we encountered many patients with encephalitis. In this year, we were not only struck by the large number of encephalitis patients but also by the diversity of their clinical picture. In this communication, we report the clinical spectrum of these patients seen during the post-monsoon period in 1998 in a JE endemic area. Patients and Methods In 1998, all the patients presenting with encephalitic illness during the post-monsoon period have been evaluated retrospectively in this study. Encephalitis was defined as acute onset of headache, fever and altered sensorium in which malaria, bacterial and fungal meningitis have been excluded. The patients were subjected to a detailed clinical evaluation. Consciousness was assessed by 15 point Glasgow coma scale (GCS)4 and muscle power on a 0-V MRC (Medical Research Council) scale. Muscle tone was classified into reduced, normal or increased. Tendon reflexes were classified into absent, reduced, normal or exaggerated. Depending on the consciousness level, the sensations were tested for pinprick, touch, joint position, vibration and cortical sensations. The extrapyramidal signs such as rigidity, dystonia, dyskinesia, tremor and other movement disorders were also noted. Cranial CT scan was carried out using a high resolution CT scanner. Parallel to orbitomeatal line, 10 mm axial sections were obtained. Cranial MRI was carried out in all the patients on a 2T scanner operating at 1.5 T (Magnetome, SP, Siemens Germany). T1 (500/15/3- TR in ms, TE in ms/excitations), proton density (2000-2500/15-20/1) and T2 (2000-2500/80-90/1) weighted spin echo sequences were obtained. Electroencephalography was carried out on a 10 or 18 channel electroencephalograph using a 10-20 system of electrode placement. Parasagittal, temporal and transverse montages were recorded using bipolar and referential derivations. Response to intermittent photic stimulation varying from 3-30 Hz, passive eye opening and cutaneous stimulation were recorded. The EEG recording during hyperventilation, eye closure and opening were carried out in the patients who could cooperate. A 30 min EEG recording was obtained in all the patients. The EEGs were analyzed for background activity, any asymmetry in voltage and frequency, rhythmic activity and epileptiform discharges.5 Central motor conduction time to abductor digiti minimi (ADM) and tibialis anterior (TA) were recorded bilaterally in all the patients using standard techniques. Median and tibial somatosensory evoked potentials were also carried out bilaterally employing standard techniques and compared with normative data of our laboratory.6 All the patients were subjected to blood counts, hemogram, urinalysis, serum chemistry and blood smear examination for parasites. Cerebrospinal fluid was examined in all the patients for protein, sugar, cells, bacteria and fungi. Laboratory test for JE virus infection included hemagglutination inhibition (HI) titres against JE virus in acute and convalescent sera, MAC ELISA and isolation of JE virus. In the patients in whom only one serum sample was available these were screened for JE specific IgM hemagglutination inhibition antibody by testing before and after treatment with mercaptoethanol (2 ME) test. A fourfold rise of HI titre or positive MAC ELISA or 2 ME test or isolation of JE virus was considered diagnostic of JEV encephalitis.7,8 On the basis of these virological studies, the patients were grouped into (A) JEV encephalitis and (B) non-specific encephalitis. On the basis of radiological findings the patients with thalamic and/or basal ganglia involvement were included in group I (15 patients), those with isolated brainstem involvement in group II (3 patients) and those with normal MRI in group III (8 patients). The clinical, neurophysiological and the results of laboratory studies have been compared in these groups of encephalitis patients. The outcome of the patients was defined at the end of 3 months into poor (bedridden state), partial (dependent for activity of daily life) and complete recovery (independent for activities of daily living).6 Results During 1998, we managed 5 patients with pyogenic meningitis, 9 with cryptococcal meningitis, 15 with tubercular meningoencephalitis and 27 with viral encephalitides. One of the patients with viral encephalitis was due to herpes simplex type I which was diagnosed on the basis of characteristic clinical, EEG, MRI and PCR. The remaining 26 viral encephalitis patients were seen during May and November and they hailed from the JE endemic area 3 of the state of Uttar Pradesh and Madhya Pradesh of India and Nepal. All of them belonged to rural areas, 10 were females and 4 children were below 13 years of age. The patient with herpes simplex encephalitis will not be discussed further. 14 patients had virological or serological evidence of JEV infection and in 12 patients there was no such evidence and the latter have been grouped as non-specific encephalitis. The clinical, radiological and neurophysiological findings of these two groups of encephalitis patients are mentioned in Table 1. The patients with JEV encephalitis had more severe illness as evidenced by lower GCS score, higher frequency of anterior horn cell involvement, movement disorders and more extensive MRI changes. The EEG and MEP changes were also more frequently abnormal in the JEV group. The distribution of the clinical, neurophysiological and laboratory findings of these patients are presented in Table 1. In group I, 13 patients had bilateral thalamic involvement (Figure 1) and 2 had basal ganglia involvement (Figure 2) of whom 1 had associated parietal cortex involvement. In the patients with thalamic lesions, basal ganglia was also involved in 6, midbrain in 10, pons in 2 and cerebellum and temporal cortex in 1 patient each. These patients had more severe illness manifested by deep coma (mean GCS= 7.4, range 3-15), high frequency of seizures (7 patients), presence of focal weakness (12 patients) and movement disorders (10 patients). 11 patients had quadriplegia and 1 hemiplegia. Tendon reflexes were reduced in 3, increased in 3 and a mixed pattern was present in 7 patients. As the patient recovered from coma, a wide variety of movement disorders were noted in 10 patients which included parkinsonian features in 8, abulia in 8, dystonia in 5 and chorea in 1 patient. Significant proteinuria exceeding 300 mg/day was present in 10 patients and exceeded 3 gm/day in 1. 2 of these patients were admitted in Nephrology department due to renal failure and 1 underwent hemodialysis. Serum bilirubin was raised in 4 patients and ranged between 1.2 and 9.6 mg%. Serum transaminase values were elevated in 11 patients, and exceeded 4 times the normal in 3. CSF was abnormal in 9 patients; mean CSF protein was 82.6 (range 16-397) mg/dl and mean cell count 73 (range 0-930)/mm3 and sugar 63.3 (range 10-150) mg /dl. EEG was abnormal in 15 patients and revealed diffuse slowing of delta to theta range. Epileptiform activity was present in 1 patient only. Motor evoked potentials were abnormal in 10 out of 13 patients (23 limbs; unrecordable in 13 limbs). SEPs were abnormal in 1 out of 11 patients only; in this patient, both median and tibial SEPs were unrecordable and he died. Evidence of anterior horn cell involvement manifested by fibrillations on EMG was present in 4 patients. Laboratory evidence of JE virus infection was present in 11 out of 12 patients in whom these were carried out. Fourfold rise in HI titres was present in 5 patients. MAC ELISA was positive in 2, 2 ME (mercaptoethanol test) was positive in 4 and JE virus was isolated in 2 patients. In this group, 4 patients died, 3 had poor, 1 partial and 7 good outcome. Three patients had isolated midbrain involvement on MRI which constituted group II (Figure 3). One of these patients developed severe respiratory paralysis and died on the 10th day of illness. In this patient, the neurophysiological studies were not possible. In the remaining 2 patients, GCS was 7 and 1 had external opthalmoplegia. Tendon reflexes were brisk in 1 and of mixed pattern in the other. Both of these patients had parkinsonian features and 1 had jaw opening dystonia and the other patient had myoclonic jerks in the lower limbs. Both these patients had abnormal CSF and recovered completely. Laboratory evidence of JEV infections were lacking in this group. In group III (normal MRI) there were 8 patients. The clinical picture was characterized by milder degree of unconsciousness (Mean GCS 12.4, range 7-15) as compared to group I. Behavioral abnormality (delirium) was present in 7 patients and seizure in 2. None of these patients had focal weakness although tendon jerks were exaggerated in 3 patients. 5 of these patients had movement disorders which included parkinsonian features in 3, abulia in 1, dystonia in 1 and perioral tongue and jaw tremor in 1 patient. The severity of these movement disorders was less as compared to group I. Significant proteinuria although was present in 3 patients but serum creatinine was raised in 1 patient only. Liver dysfunction was the presenting symptom in 2 patients, whose serum bilirubin was high, 8 and 2.4 mg/dl respectively. Serum transaminase was elevated in 5 patients, and exceeded 4 times the normal in 1. CSF was abnormal in 2 patients only, 1 had high protein (181 mg/dl) and the other had lymphocytic pleocytosis (25/mm3). At 3 months follow-up, all these patients had complete recovery. Laboratory evidence of JE was present in 3 patients and included virus isolation and positive MAC ELISA in 1 patient each, and four-fold rise of HI titre in convalescent sera was present in another. The clinical, radiological and neurophysiological findings of these groups are summarized in Table 2. Discussion An analysis of 26 patients with endemic encephalitis during May to November in 1998 in a tertiary care centre in India revealed a wide spectrum of clinical, neurophysiological and MRI findings. Laboratory evidence of JEV infection was present in 14 patients. Comparison of JEV encephalitis patients with those without evidence of JEV infection revealed somewhat similar findings; although the patients with JEV group had more severe illness. Japanese encephalitis results in widespread involvement of the nervous system. On MRI, thalamus, basal ganglia and brainstem involvement are common and thalamic involvement has been reported to be suggestive of JE in an endemic area, especially in the post-monsoon period.6 In JE, the cerebellum, cerebral cortex and spinal cord is also affected to a variable extent.9,10 A similar distribution of MRI changes with high frequency of thalamic and basal ganglia involvement has been reported in eastern equine encephalitis from USA. Thalamic and basal ganglia involvement was reported in 71% patients each and brainstem in 43%.11 The clinical and radiological findings in encephalitis are generally non-specific and should be interpreted in the geographical and other epidemiological background. Patients with isolated brainstem involvement had no laboratory evidence of JEV infection. Brainstem encephalitis is known to occur in listeria monocytogenes, mycoplasma, St Louis encephalitis and cytomegalovirus infection.12-14 In JE, brainstem involvement has been reported on the basis of MRI and autopsy studies.9,15,16 On classifying our patients on the basis of MRI findings and comparing the clinical, neurophysiological and virological findings in different subgroups, there was an overlap of results. Anterior horn cell involvement in JE has been reported on the basis of autopsy and neurophysiological findings.10,15 In the present study, the evidence of anterior horn cell involvement was present in both JEV encephalitis and non-specific encephalitis as evidenced by focal wasting, reflex loss and/or denervation on electromyography. In the patients with normal MRI, however, there was no evidence of anterior horn cell involvement and these patients recovered well. In our patients, a high frequency of renal and hepatic dysfunction was noted. The renal dysfunction was evidenced by proteinuria and raised serum creatinine levels. Liver dysfunction manifested with raised serum bilirubin and transaminase levels. The impairment of kidney and liver functions was more frequent in the patients with JEV encephalitis. In the published literature kidney and liver dysfunctions have not been reported in JEV encephalitis patients. We had excluded the common causes of liver dysfunction in these patients such as malaria, hepatitis B and C. In experimental JEV infections, minimal inflammatory response in liver has been reported. Liver revealed swollen Kupffer's cells, some of which showed karryorrhaxis.17 Hematuria and albuminuria have also been reported in the acute stage of JE.18 In an experimental study ultrastructural changes in the kidney have been reported following JEV infection.8 Occurrence of encephalitis in the post-monsoon period in JE endemic areas and overlapping clinical, radiological and neurophysiological findings in our patients suggest the role of JE or JE-like viruses. Japanese encephalitis virus infection has a wide clinical spectrum which may range from subclinical infection to febrile headache syndrome, aseptic meningitis and varying severity of encephalitis. The observed diversity of clinical manifestation in our encephalitis patients may be due to strain variation, change of virulence of virus or alteration in host immunity. Further studies are needed to elucidate the basis of such a wide clinical spectrum of JE. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03011f1.jpg] [ni03011t1.jpg] [ni03011t2.jpg] [ni03011f3.jpg] [ni03011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}