 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
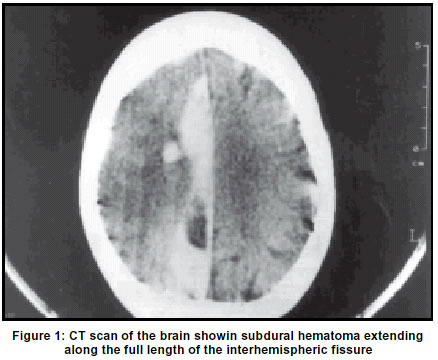
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 63-64 Case Report Interhemispheric subdural hematoma: An uncommon sequel of trauma A. Shankar, M. Joseph, M. J. Chandy Department of Neurological Sciences, Christian Medical College and Hospital, Vellore, Tamil Nadu-632004, India. Accepted on 22.01.2001. Code Number: ni03013 Interhemispheric subdural hematomas are relatively uncommon and usually seen in patients with bleeding disorders. They may present with signs of the falx syndrome or seizures. The management options range from craniotomy and evacuation to conservative management. We report such a case in a patient with normal bleeding parameters, which was managed with a twist drill craniostomy and drainage of the hematoma. Key Words: Interhemispheric, Traumatic, Subdural hematoma. Interhemispheric subdural hematomas, first described by Aring and Evans1 in 1940, constitute a rare type of subdural hematoma with only about 100 cases reported till 1997.2-5 They are usually considered to be a distinct entity because of their unusual location and the fact that their management is still a matter of debate. A recent case is reported and management options are reviewed. Case Report A 65-year-old lady presented three days after a fall on level ground. She had been asymptomatic for a day following the fall, but then developed left-sided hemiparesis and altered sensorium, which worsened over a few hours, to become static till admission 48 hours later. There was no history of seizures or vomiting. She had suffered from an acute diarrhoeal disorder for two days prior to her injury. On examination, she was dehydrated but hemodynamically stable. Her Glasgow Coma Scale was 13/15 (opening eyes to call, obeying commands and confused). Pupils were both equal and reacting, but fundi could not be visualized due to the presence of cataract. She had a left upper motor neuron type of seventh nerve paresis and a left hemiparesis with grade II power. Deep tendon reflexes were exaggerated and plantar was upgoing on the left side. A CT scan of the brain showed a 1 cm thick subdural hematoma extending along the full length of the interhemispheric fissure (Figure 1). In addition, there was a thin right frontal subdural hematoma, and two small right frontal contusions - one in the convexity region and a second one postero-medially, in the region of the centrum semiovale, adjacent to the body of the lateral ventricle. All the hematomas were hyperdense, with a small loculated hypodensity in the interhemispheric fissure. Her biochemical studies were within normal range. As her neurological condition had been stable for over 48 hours, she was treated conservatively with anticonvulsants, anti-edema measures and fluid replacement. Her sensorium remained stable over the next 2 days. However, on the third day, it was found that she was opening eyes only to pain, and was only localizing pain and making incomprehensible sounds (GCS Score 9/15). The power in the left upper and lower limbs had deteriorated to grade I. A repeat CT scan of the brain showed increase in the perilesional edema, but there was no change in the size of the hematoma. A paramedian twist drill craniostomy was done just anterior to the coronal suture and approximately 15 ml of dark altered blood clot was evacuated, following which her neurological condition improved. Discussion Interhemispheric subdural hematomas are uncommon lesions, usually occurring in patients with bleeding diatheses.2 They are associated with trauma in 83% of cases.3 Other reported causes include child abuse with shaking, forceps delivery or a history of birth trauma, hemodialysis, anticoagulation, aneurysmal bleeding6 and penetrating injuries. The preceding trauma is frequently of low velocity, and injury to the bridging veins of the interhemispheric fissure is believed to be the cause of the hematoma. However, the vector of force that can produce an interhemispheric subdural hematoma remains controversial. Fruin et al7 postulated that an occipital blow in the sagittal plane would lead to an interhemispheric subdural hematoma because of the anatomic orientation of the veins in the interhemispheric fissure, which tend to course antero-medially from the cortex to the midline sinuses. These lesions are usually unilateral, but bilateral hematomas have been reported.8 List9 first described the falx syndrome in patients with interhemispheric subdural empyemas in 1955. Patients present with contralateral hemiparesis, the lower limb being involved more than the upper. Other presenting symptoms can include clouding of consciousness, focal or generalized seizures, dementia, language disorders, gait ataxia and oculomotor dysfunction.10 Conservative treatment and surgery are equally favored in the treatment of these patients11. Surgical interventions ranging from a twist drill craniostomy to craniotomy and evacuation of hematoma have been tried.12 There is no difference in outcome between those treated by burr hole evacuation of hematomas and craniotomies. Though removal of the clot has proved to be a viable option in the management of these patients, there is some danger due to the proximity of the superior sagittal sinus and bridging veins. Furthermore, some of these hematomas migrate superiorly (to a more favorable position as regards surgery) with time, as they liquefy.13 Another point in favor of conservative management is the fact that there is no significant difference in the outcomes of those treated by either modality. If at all, patients who underwent surgery had impaired consciousness for a longer period of time. Though there is no consensus on the ideal management of these rare hematomas, a flexible treatment plan has to be made, where surgical treatment is reserved for those who have pronounced symptoms or neurological deficits, and conservative treatment may be followed in those who are neurologically stable or have concurrent risk factors.2,3 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03013f1.jpg] |
| |||||||||

{kind=link}