 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
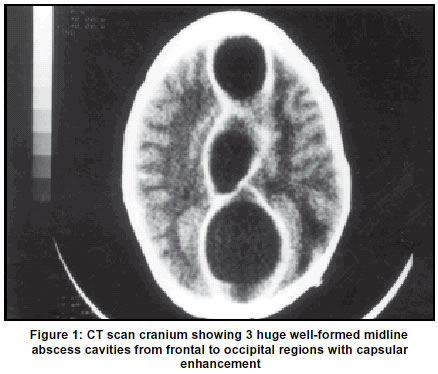
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 65-66 Case Report Massive falx cerebri empyema A. K. Yende, S. Mohanty Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, India. Accepted on 05.02.2001. Code Number: ni03014 A rare case of otogenic massive intra-falx empyema is reported. The patient presented with headache, vomiting and left lower limb weakness of 8 months duration. C.T. scan revealed two cavities in the falx. Right fronto-parietal craniectomy and drainage of massive empyema was undertaken through interhemispheric approach with wide opening of the falx, evacuation of voluminous amount of thick pus and marsupalization of flax with dura. The patient showed complete recovery. The relevant literature is briefly reviewed. Key Words: Falx cerebri, Empyema, Marsupalization, Abscess, Chronic supperative otitis media. Subdural empyema has been described in several reports.1-8 Its origin, clinical course, radiological appearance and treatment have been well established. There are no reports of massive intra-falx empyema with multiple cavitation. Case Report A 10-year-old male child presented with recurrent episodes of high grade fever, headache, vomiting and left leg weakness for 8 months. He had one episode of focal seizure eight months ago involving the face. The child had purulent otorrhoea for 5 years. He was irritable and had positive signs of meningeal irritation. He had bilateral papilloedema, and right-sided upper motor neuron type of facial paresis. He had conductive deafness on left side. CT scan showed a large interhemispheric abscess (Figure 1). A fronto-parietal craniectomy and drainage of massive falx cerebri empyema cavities was done through right interhemispheric approach Superior sagittal sinus was thrombosed at its middle. Abscess cavity was bulging maximum between layers of falx at its middle. It was opened up and thick yellowish green purulent pus was drained out. About 150 ml pus was drained and the abscess cavity was thoroughly irrigated with normal saline mixed with gentamycin. The abscess wall i.e. falx was marsupalized with silk sutures to the dural opening. Patient was subsequently treated with appropriate antibiotics. Discussion Abscess in subdural space usually arises as a complication of nearby infections in paranasal sinuses and the middle ear and less commonly, follows a penetrating wound, bullet injury, or as a complication of therapeutic procedures, e.g. intracranial pressure monitoring, craniotomy and after drainage of subdural hematoma.6 Headache, fever and neck stiffness occur early in these patients. Seizures, usually of focal type, can occur. Many patients deteriorate rapidly over a period of hours or days. Profound neurological deficit and death can occur rapidly as the process involves thrombosis of underlying cortical veins but meningitis rarely complicates the infection.1 Subdural empyema represents 13-20% of all intracranial suppurations. About 9% children with brain abscess have associated subdural empyema about 1h-3 to 1/2 of patients are below the age of 20 years. Almost 80% of subdural empyema occurred over convexities and 12% in the interhemispheric fissure. However, the spindle shape of the empyema on CT was determined by the confining boundaries of neovascularization in the abscess capsule and compression of cerebral tissues on the other. Hypermia in normal adjacent brain also plays a role in outlining the interhemispheric mass. Abscess within the leaves of the falx has never been reported. Usually, the empyema collect below and to either side of the falx.4,5 Superior saggital sinus may be displaced away from the inner table of the skull. The thrombosis of the sinus as was observed in our case is rare. The only method of treatment is wide exposure, evacuation of the pus and thorough irigation of the region with antibiotic solution. Heavy encapsulation does not occur and at times a portion of the thin-walled capsule may have to be left adherent to vital areas of the cerebral cortex. All infectious material, whether purulent or granulation tissues, must be removed. They are often multiloculated and care is to be taken to make sure that all pockets are drained which can be confirmed by serial CT scans performed postoperatively. Appropriate antibiotics should be continued systemically for 3-4 weeks.1,6 Mortality still remains high (25-38%) and appears to be influenced by age of the patient, preoperative course of the disease, etiological factors, preoperative neurological state, localization, diagnostic failures and postoperative complications.3,4,6 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03014f1.jpg] |
| |||||||||

{kind=link}