 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
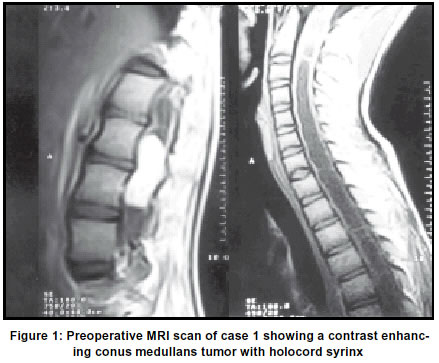
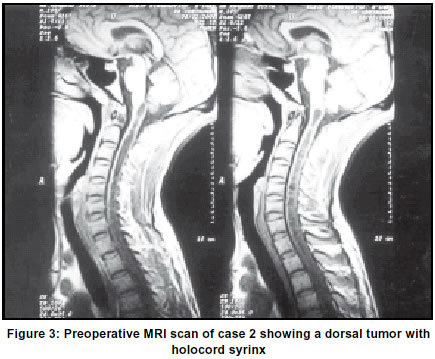
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 67-68 Case Report Secondary holocord syringomyelia with spinal hemangioblastoma: A report of two cases S. B. Pai, K. N. Krishna Department of Neurosurgery, M. S. Ramaiah Medical College, Gokula Extension, Bangalore-560054, India. Accepted on 09.02.2001. Code Number: ni03015 Intramedullary spinal hemangioblastoma is well known to be accompanied by syringomyelia. However, holocord secondary syringomyelia is uncommon. We present 2 cases of spinal hemangioblastoma, one in the conus medullaris and the other in midthoracic region, accompanied by holocord syrinx. In both the cases the secondary syrinx resolved following successful total tumor excision with good neurological recovery. Key Words: Holocord syrinx, Conus medullans tumor, Spinal hemangioblastoma, Secondary syringomyelia. Spinal hemangioblastomas are highly vascular tumors which may be totally solid or have a cystic component. They constitute 1.6% to 2.1% of all primary spinal cord tumors1 and are usually located in the cervical and thoracic region.2 Secondary syringomyelia may present in association with spinal cord tumors, infarction, inflammatory processes, trauma, etc. Intramedullary tumors are well known to be associated with accompanying syringomyelia. Ependymomas and hemangoblastomas are the most common tumor types associated with syrinx.3 More than half the cases of spinal hemangioblastomas are accompanied by a syrinx.4 Case History Case 1A 17-year-old male presented with progressive quadriparesis and bladder involvement. On admission, he had flaccid quadriplegica with sparing of the diaphragm and had an indwelling bladder catheter. MRI of the spine revealed a lobulated mixed intensity contrast enhancing mass with areas of flow void in the region of the conus medullaris with a syrinx occupying almost the entire spinal cord from C2 to the conus medullaris, i.e. holocord syrinx (Figure 1). The whole spinal cord and the posterior fossa were screened after contrast to confirm the absence of any other tumor or lesion. Investigations for VHL disease were negative. At surgery, a large (4.5 cm x 2.0 cm) cherry red highly vascular tumor involving the conus medullaris and the filum terminale with an exophytic component was noted. The upper margin of the tumor was opening into the syrinx cavity above. The tumor was excised in completely using standard microsurgical techniques. Histopathological examination confirmed that it was a hemangioblastoma. In the immediate postoperative period patient started making rapid neurological recovery. 18 months later, he had recovered the power in all 4 limbs totally with very minimal hypertonicity and no sensory disturbance. He was back to his normal routine with an incomplete bladder recovery as the only residual deficit. Repeat MRI confirmed total excision and no recurrence of the hemangioblastoma, the syrinx had collapsed (Figure 2). Case 2A 35-year-old male presented with dysaesthetic pain in both the lower limbs with progressive paraparesis of 6 months duration. Examination revealed normal spine with spastic paraparesis and bilateral hand grip weakness. Deep tendon reflexes in the upper limbs were depressed and exaggerated in the lower limbs. There was dissociated sensory loss in the upper limbs and on the trunk up to D7 level and global sensory loss below D7. Investigations revealed a 2.4 cm x 1.6 cm sized mixed intensity intramedullary lesion with flow voids on the surface at D8 level accompanied by a holocord syrinx extending above and below that level (Figure 3). At surgery a hemangioblastoma was completely excised. In the immediate post operative period the patient showed good recovery of power and sensations in the upper limb. However, no neurological recovery in the lower limbs was observed at the end of the first postoperative month. Discussion Syringomyelia is frequently associated with intramedullary tumors, especially ependymomas and hemangioblastomas. Two main mechanisms have been postulated for the development of syringomyelia in intramedullary tumors. Transudation of fluid from the pathological tumor vessels is believed to be the main cause of the syrinx. However, obstruction to CSF flow and extracellular fluid flow is also said to play a role in the formation of syrinx, which is more often seen above the tumor than below it. It is postulated that the subarachnoid space and the extracellular space are a single fluid compartment with interrelated fluid flow. A block in one of the spaces will be reflected as an increased flow in the other. The higher the level of the tumor the greater the incidence of the accompanying syrinx.3 Magnetic Resonance Imaging with contrast (Gd-DTPA) is the investigation of choice for intramedullary tumors with syringomyelia.5,6 Associated syrinx favors resectability of the tumor and these patients recover from surgery sooner.7,3 No specific treatment of the syrinx is necessary and the syrinx usually resolves with excision of the tumor.7 On review of literature we could not find any report of a conus medullaris tumor with a holocord syrinx. With microneurosurgical techniques, complete removal of the tumor is possible in most cases.7-9 To our knowledge, a patient with a conus medullaris tumor and an accompanying holocord syrinx has not been reported so far. It appears that due to the large exophytic component and a capacious canal in the lumbar region, neurological manifestation was delayed in this patient. Secondary syrinx in this patient is probably due to the transudation of fluid from the tumor vessels rather than due to a block in the CSF pathway since the tumor was in the conus medullans. In the second patient both transudation of fluid as well as obstruction to CSF flow could have caused the syrinx which was found both below and above the tumor. The early neurological recovery in both the cases was due to the resolution of the secondary syrinx. Acknowledgements The authors wish to acknowledge with gratitude the efforts of Mrs. Rukmini and Mr. Mohan for secretarial and library assistance. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03015f2.gif] [ni03015f1.jpg] [ni03015f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}