 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
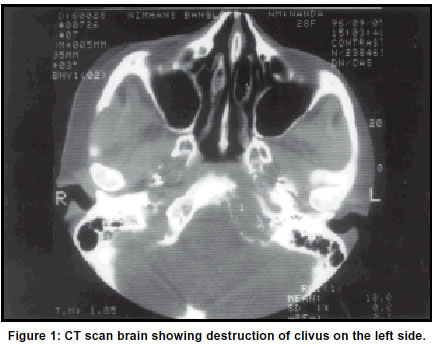
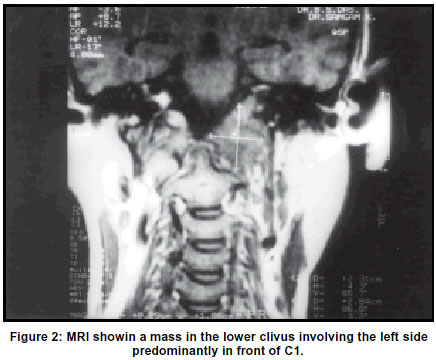
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 69-70 Case Report Tuberculous osteitis of clivus B. Indira Devi, A. K. Tyagi, D. I. Bhat, V. Santosh* Department of Neurosurgery and *Neuropathology, NIMHANS, Bangalore-560009, India. Accepted on 10.03.2001. Code Number: ni03016 Tuberculous osteitis of clivus is rare. Its diagnosis is difficult because of the rarity of the site and the non-specific nature of the disease. Management consists of confirmation of diagnosis by biopsy and chemotherapy with anti-tubercular drugs. Meningitis may complicate the clinical course, increase morbidity and mortality. Key Words: Tuberculous osteitis, Cranial nerve palsies, CT scan, Transoral biopsy. Tuberculous ostetitis of the skull base is rare. The usual clinical picture is of jugular foramen syndrome. Additional neurological deficits are due to either extensive skull base involvement or due to meningitis. In the presence of tubercular infection elsewhere in the body or in an endemic region, the etiology of osteitis can be presumed to be tubercular. We describe a case of tuberculous osteitis of the skull base where the clinical picture kept changing even on presumptive treatment with antitubercular drugs. Diagnosis could be confirmed by transoral biopsy. Report A 28-year-old female presented with diffuse neck pain and headache for 10 days and double vision and blurring of vision for 8 days. There was past history of episodic left-sided headaches. There was history of left-sided weakness of face of 8 months duration and deviation of tongue to left and dysphasia for the same duration. Examination revealed an alert healthy female patient. She was afebrile and there were no meningeal signs. She had bilateral lateral rectus palsy and left-sided facial weakness. The tongue was deviated to the left and there was mild wasting. Rest of the neurological examination was normal. She was seronegative for HIV. Total leucocyte count was 17000/cmm, ESR was 30 mm at the end of one hour, liver function tests and renal function tests were within normal limits. Lumbar puncture and CSF examination showed 700 cells/cmm (95% lymphocytes, 5% polymorphs), glucose 30 mg, proteins 180 mg%, Elisa positive for IGH SIGIN. Plain X-ray skull basal view showed destruction of left lateral pterygoids, clivus and petrous. CT scan revealed destruction of clivus on the left side. MRI T1 and T2 weighted images showed a mass in the lower clivus involving the left side predominantly in front of C1. Patient was started with presumptive treatment with anti tubercular drugs INH 300 mg od, Rifampicin 450 mg, Pyrazinamide 1000 mg od, Pyredoxine 10 mg od and steroids. Three weeks later she developed pain and tenderness first over lumbar spine then over the dorsal spine and finally over the cervical spine over days. Examination revealed, mild hypotonia in all the muscles, power in upper limbs was 4/5 at shoulders, 3/5 at elbow and wrist; power in the lower limbs was lIS in all the groups. Patient was aflexic. There was no sensory loss, bladder and bowel were normal. At this stage patient was investigated with plain x-rays of lumbar and cervical spine and myelogram with IOHEXEOL was done. There was no evidence of compression of the cord. A decision to obtain histological diagnosis of the clival lesion was made since the patient had a changing and progressively deteriorating neurological picture and the possiblity neo-plastic lesion with paraneoplastic disorder could not be ruled out. A transoral transpharyngeal biopsy of the clival lesion was done. At surgery a yellowish gray lesion destroying the clivus was seen superior to anterior arch of CI on the left side. Histological diagnosis was tubercular granuloma infiltrating the marrow of clivus. Post operative course was uneventful. Patient did not make any improvement in lower limbs. She was discharged two weeks later on anti-tubercular treatment for 18 months. At the follow up a year later, she was walking with support, power in the lower limbs had improved to grade 4/5 proximally,3/5 distally. There were no fresh deficits. Follow up MRI scan was not done. Final diagnosis in this patient was tubercular osteomyelitis of the clivus with possible spinal arachnoiditis secondary to spinal meningitic process. Discussion Skull involvement in tuberculosis is very rare. Most of the reported cases are anecdotal.1-3 It appears to be more common in childhood and in the pigmented races.2-5 Though infection with immune-deficiency virus has once again caused a rise in the prevalence of tuberculosis in general, tubercular osteitis of the skull does not seem to be on the increase.5-7 Tuberculous osteitis of the skull base is rare. In the few reported cases, the skull base was involved in contiguity, either from the mastoids or the middle ear, or the paranasal sinuses or from the convexity.2 Presence of tubercular infection else where in the body, e.g. lungs may help in diagnosing the skull base involvement. The clinical symptomatalogy of osteomyelitis of the skull base of any etiology is unilateral, headache and jugular foramen syndrome.8 Additional neurologic deficits are due to local or generalized meningitis. Meningitis was reported in 10 of 233 cases of osteitis in the Strauss series, 1 of 4 in Ganguli and Witcombe series.1,2,5 Prognosis worsens with the onset of meningitis. Multiple cranial neuropathies are due to meningitis resulting in local ischemia, due to entrapment of the nerves in exudate or due to endarteritis. The neurologic deficits generally recover to a large extent with steroids and antitubercular treatment. Our patient had meningitis with changing and progressively worsening paraparesis without sensory or sphincter involvement. This can be explained by anterior spinal artery involvement or by compression of ventral medulla by clival osteomyelitis. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03016f1.jpg] [ni03016f2.jpg] |
| |||||||||

{kind=link}
{kind=link}