 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 77-78 Case Report Lipoma in the region of the jugular foramen A. V. Prasanna, D. P. Muzumdar, A. Goel Department of Neurosurgery, King Edward Memorial Hospital, Parel, Mumbai-400012, India.
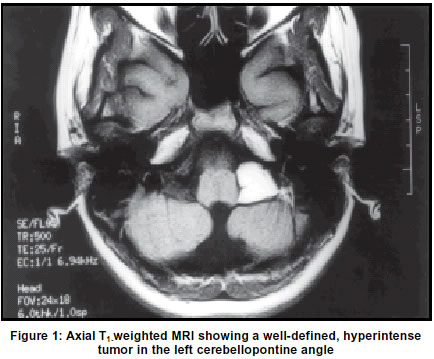
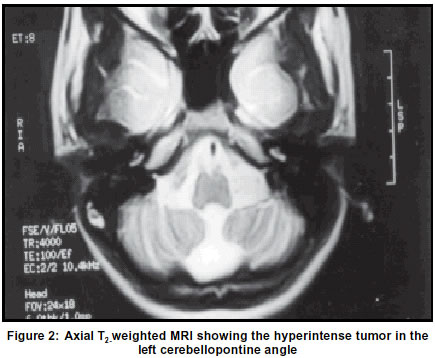
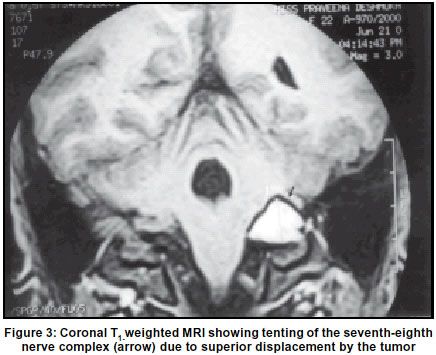
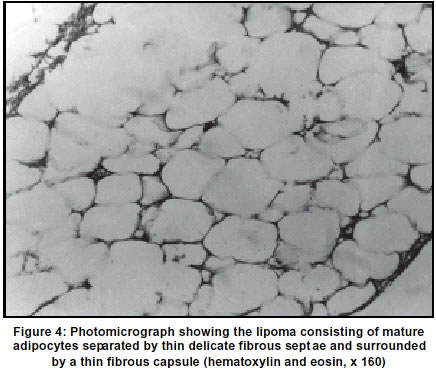
Accepted 04.05.2001. Code Number: ni03020 A 22-year-old girl presented with a gradually progressive loss of hearing in the left ear and ipsilateral facial paresis. Investigations revealed a lipoma in the region of the jugular foramen. Conservative resection of the tumor resulted in improvement in facial paresis. The treatment options in such cases are discussed in this report. Key Words: Lipoma, Jugular foramen, Cerebellopontine angle. Although rare, lipomas can occur at the cerebellopontine angle and account for approximately 0.5% of all intracranial tumors.1 Computerized tomography (CT) scan and magnetic resonance imaging (MRI) along with fat suppression images, provide a reasonably clear diagnosis.2 The benign nature, extremely slow rate of growth and difficulty in radical resection of the tumor when in the vicinity of cranial nerves, are the factors that need to be critically evaluated when planning surgery. The literature on the subject is briefly reviewed and the surgical options are discussed. Case report A 22-year-old female presented with complaints of slow progressive loss of hearing in the left ear for about 10 years. During the same period she noticed a slow progressive weakness of the left side of the face. She had a subcutaneous lipoma in the occipital region. On examination there was moderate (House-Brackmann Grade II) left infra-nuclear facial nerve weakness and deafness in the left ear. MRI of the brain showed a hyperintense lesion on both T1 and T2-weighted images (Figures 1 & 2) in the region of the jugular foramen. The image characteristics were suggestive of lipoma. The lesion was explored through a left retromastoid route. A subcutaneous lipoma measuring approximately 2.5 cm in diameter was excised as it was in the line of the incision. The lipoma in the cerebellopontine angle was found merged with the lower cranial nerves and posterior inferior cerebellar artery and indented the seventh-eighth nerve complex from below (Figure 3). The tumor was relatively firm and elastic. As the lower cranial nerves were clinically normal and the tumor could not be dissected from the lower cranial nerves, tumor resection was done with the aim to decompress the seventh-eighth nerve complex. The tumor in the vicinity of these nerves was removed and no attempt was made to remove the tumor in the region of the lower cranial nerves. Her facial nerve paresis improved remarkably within a week of surgery to complete normalcy. However, her hearing did not improve. Histological examination revealed a tumor consisting of mature adipocytes separated by thin delicate fibrous septae. It was surrounded by a thin fibrous capsule (Figure 4). Discussion Intracranial lipomas are developmental malformations and originate from metaplasia of a persistent meninx primitiva in the subarachnoid cisterns.3 The commonest intracranial location of these tumors is in the pericallosal cistern, where it accounts for approximately 50% of the intracranial lipomas.4 The tumor in the pericallosal cistern is usually associated with corpus callosal agenesis, suggesting a congenital origin.5 Cerebellopontine angle lipomas are rare and constitute less than 0.14% of all cerebellopontine angle tumours.6 Most of the reported cases have an association with the internal auditory meatus.7 Lipomas which merge into the lower cranial nerves and compress the seventh-eighth-nerve complex have not been reported so far. These tumors are histologically benign and have an indolent course.4,7 They present with subtle and progressive symptoms over several years. On our literature search, we could locate only one report of an intracranial lipoma which was associated with the presence of an additional subcutaneous lipoma.8 The pathogenic association of these lipomas at two distinct sites could not be confirmed. However, presence of multiple lipomas suggests a common mode of origin. CT scan and MRI features are characteristic for lipoma but they can be confused with an epidermoid or a dermoid tumor. Fat suppression on MRI can help clarify the diagnosis.2,3 In the presence of progressive symptoms, surgical decompression appears to be the best option. However, an incidentally detected lesion can safely be observed. Although a radical surgical resection can be expected to cure these lesions, resection in the vicinity of the lower cranial nerves may not be easy or advisable, particularly when these nerves are functionally intact.7,9 The tumor merges into the adjoining structures and some of them can even be vascular. These factors can limit the extent of surgical resection. Despite the encasement of the lower cranial nerves in our case, these nerves were functionally normal, whilst the moderate displacement of the seventh-eighth nerve complex resulted in relatively significant neurological dysfunction. This feature may reflect the relative tenacity of the lower cranial nerves and relative vulnerability of the seventh-eighth nerve complex. Partial resection and decompression of the seventh-eighth nerve complex in our case resulted in gratifying improvement of the facial nerve function. In the presence of progressive symptoms, surgical decompression appears to be a reasonable option. The rate of growth of lipomas is extremely slow and the long-term outcome is excellent.4 References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03020f3.jpg] [ni03020f1.jpg] [ni03020f4.jpg] [ni03020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}