 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
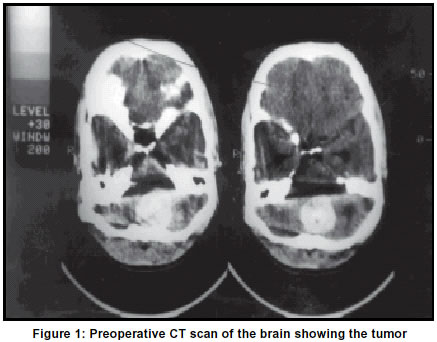
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 79-80 Case Report Foramen magnum metastatic malignant melanoma S. B. Pai, K. N. Krishna Department of Neurosurgery, M. S. Ramaiah Medical College, Gokula Extension, Bangalore-560054, India. Accepted on 13.06.2001. Code Number: ni03021 The foramen magnum as a site for brain metastasis is extremely rare. We report the case of a 24-year-old male who presented with features of increased intracranial pressure and lower cranial nerve palsies. Imaging revealed a foramen magnum tumor with extension up to the cerebellar vermis superiorly and into the spinal canal inferiorly (craniospinal mass) with mild obstructive hydrocephalus. A malignant melanoma was completely excised. The patient continued to be tumor-free 24 months later. Key Words: Craniospinal tumor, Malignant melanoma, Brain metastases, Foramen magnum. Brain metastases usually occur through the hematogenous route and the common primary sources are lung, breast, uterus, intestine, kidney and thyroid. Malignant melanoma accounts for about 12% of brain metastases.1 Most of the metastatic deposits occur in the cerebrum (80%).1 The craniospinal junction or foramen magnum is an extremely uncommon site for metastasis. We report a rare case of a foramen magnum metastatic malignant melanoma with cranial and spinal extension. Case Report A 24-year-old male presented with headache, vomiting and change in voice of two weeks duration. On examination he was found to have bilateral severe papilloedema, lower cranial nerve palsies and severe truncal ataxia. A CT scan of the brain revealed a hyperdense well-circumscribed mass in the region of the cerebellar tonsils extending inferiorly into the posterior spinal canal with mild obstructive hydrocephalus (Figure 1). MRI scan delineated the lesion much better showing the lower limit and lateral extension to the left jugular foramen. The radiological features were suggestive of an extraaxial intradural tumor like a cranial nerve schwannoma or meningioma. The hematology, biochemical investigations and chest X-ray were normal. The patient was subjected to suboccipital craniectomy and C1C2 laminectomy. At surgery ligamentum nuchae and the exposed dura were found to be blackish. On opening the dura mater an extramedullary subarachnoidal tarry black tumor which could be freed from the neural tissue was found and totally excised. Histopathological examination revealed a malignant melanoma. Postoperative period was uneventful and no primary site of the tumor could be found. Repeat CT scan of the brain confirmed total excision. The patient was started on radiotherapy which he discontinued. Patient improved in his neurological status and at 24 months follow-up he was ambulant with mild cerebellar signs and was free from symptoms and signs of raised intracranial pressure and lower cranial nerve palsies. Discussion The common neoplasms which metastasize to the brain arise from the lung, breast, kidney, intestine, prostate, thyroid and melanomas. Malignant melanomas account for about 12% of the secondary tumors of the brain.1 Malignant melanoma commonly metastasizes to the lung and liver. However, brain metastasis is not uncommon constituting, 12% to 20% in clinical studies and about 50% in autopsy studies. These are usually single but multiple metastases are not uncommon.2 The most frequent sites are frontal and parietal lobes.2 The present case presented with an extraaxial foramen magnum metastasis which has not been reported so far. There is also a high incidence of extracerebral metastasis at the time of diagnosis of cerebral involvement, which was not evident in our patient.3,4 The interval from diagnosis of the primary to cerebral metastases varies from 6 to 60 months.4,5 The clinical presentations depend on the site of involvement. Malignant melanoma have a characteristic appearance on CT and MRI. They are usually seen at the grey-white junction of the cerebrum and are slightly hyperdense with moderate contrast enhancement.6 Most of the lesions show peritumoral edema.3 At times, a leptomeningeal spread may also be detected.3 On MRI, typical T1 and T2 shortening is noted due to the presence of elanin.6 These metastases are classified according to their size less than 1 cm, 1-4 cm and above 4 cm.3 Patients with leptomeningeal spread of the tumor (metastatic meningeal melanomatosis) usually test positive for the putative CSF tumor markers like fibronectin and beta 2 - microglobulin. These patients also show a rise in the IgM and IgG indices, interleukin-6 and tumor necrosis factor-alpha, indicating a local immune response.7 The reported patient had an isolated extraaxial intradural metastasis without any brain parenchymal involvement, which again is unique and therefore a preoperative diagnosis could not be made despite a typical MRI appearance. The overlying dural and ligamental involvement may suggest an intradural spread in contiguity. Patients with cerebral melanomatic metastases are usually associated with a poor prognosis, with a median survival of only 8 months.5,8 Surgery for isolated cerebral metastasis can result in neurological improvement and may also result in long- term survival but may not be of value in patients with multiple lesions and extensive extracerebral spread.2,8 Chemotherapeutic agents like dacarbazine, cisplatin, carmustine, tamoxifen and fotemustine have all been tried in different combinations and regimes with varying results. 8-12 Fotemustine is a chlorethylnitrosourea that readily penetrates the blood brain barrier and has shown a response rate upto 28%.8,9,11 Radiotherapy is offered as a palliative therapeutic procedure. One- third of patients with cerebral melanoma metastases have lesions amenable to radiosurgery.13 One patient has had a symptom-free 24 month survival only radical surgical excision alone. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03021f1.jpg] |
| |||||||||

{kind=link}