 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 81-83 Case Report False aneurysm of cavernous carotid artery and carotid cavernous fistula: Complications following transsphenoidal surgery R. Kachhara, G. Menon, R. N. Bhattacharya, S. Nair, A. K. Gupta, S. Gadhinglajkar,* R. C. Rathod* Departments of Neurosurgery, Radiology and *Anesthesiology, Sree Chitra Tirunal Institute for Medical Sciences and
Technology, Trivandrum, India.
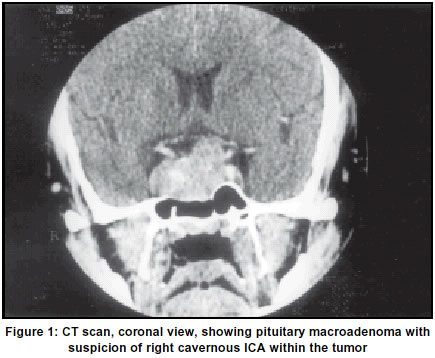
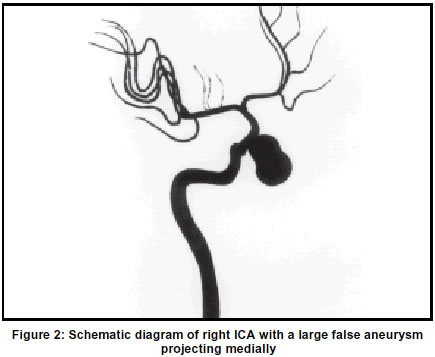
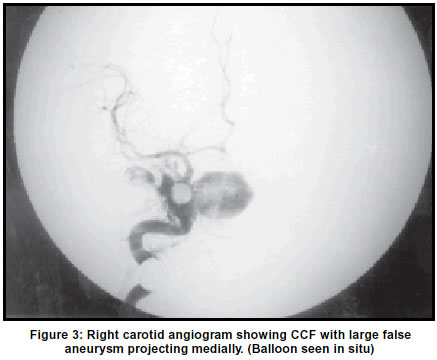
Accepted on 10.08.2001. Code Number: ni03022 We present two cases of carotid injury during transsphenoidal surgery for pituitary adenoma. While in one of the cases it resulted in the formation of a false aneurysm of cavernous carotid artery, in the other patient, a carotid cavernous fistula (CCF) formed. The false aneurysm was managed by surgical trapping and the patient had an uneventful recovery. The CCF was initially managed with balloon embolization. The balloon got deflated and resulted in a false aneurysm with persistent CCF. This was occluded with Guglielmi Detachable Coils (GDC). The management options are discussed and relevant literature is reviewed. We emphasize the importance of an early cerebral angiography to know the status of the injured carotid artery and formation of false aneurysm / fistula. Key Words: Transsphenoidal surgery, Pituitary adenoma, Carotid artery, False aneurysm, Carotid cavernous fistula. Transsphenoidal surgery has a low morbidity and mortality,1 it is nevertheless associated with potentially serious complications that should be expeditiously recognized and managed. The ability to treat the complications once they have occurred, is important in obtaining a satisfactory outcome. We report two cases of lacerations of the cavernous segment of the internal carotid artery during transsphenoidal surgery for pituitary adenoma, which resulted in the development of large false aneurysm in one patient and carotid cavernous fistula (CCF) in the other. Case Report Case 1A 40-year-old man, a manual laborer, was admitted with a 6-month history of severe bifronto-temporal headache and decreased vision in both eyes for 6 weeks. He had barely perceptible vision in the right eye at the time of presentation. He also had a history of joint pains and decreased libido. Examination revealed ptosis of the right eye. Visual acuity in the right eye was 3/60 and in the left eye was 6/60. Visual fields were severely constricted in both the eyes. The rest of the neurological examination was normal. Endocrine functions showed hypothyroidism and hypocortisolism with markedly raised prolactin levels (4010 ng / ml). Computed tomography (CT) showed an isodense mass in the sella and suprasellar region with right parasellar extention, which enhanced uniformally on contrast administration (Figure 1). In view of rapidly deteriorating vision, he underwent transnasal transsphenoidal decompression of the tumor on March 20, 2000. While incising the sellar dura on the right side, there was profuse bleeding from injury to the right cavernous carotid artery, which was controlled by packing with muscle, fascia, fat and surgicel gelfoam. He was ventilated for 48 hours along with strict control of blood pressure. CT scan revealed a thin layer of blood over the superior surface of the tumor and a small hematoma in the interpeduncular fossa. Prior to removal of the pack, an intraoperative angiogram was done which revealed a large false aneurysm of the right cavernous carotid artery, bulging into the sphenoid sinus (Figure 2). Carotid cross-compression study showed no filling from contralateral ICA but there was good cross-filling from vertebral injection. Surgical trapping of the right cavernous ICA was done. Internal carotid artery was doubly ligated in the neck and a permanent Yasargil clip was applied proximal to the ophthalmic artery via right pterional craniotomy. The hematoma on the superior surface of the tumor which caused severe optic nerve compression was evacuated. Then nasal pack was removed with removal of muscle and fascia. There was a large false aneurysm projecting in the sphenoid sinus, which was coagulated and the tumor was decompressed. The left cavernous carotid artery was also seen bulging into the sella. Hemostasis was achieved and the tumor bed was packed with fat graft. He developed pupillary asymmetry after 6 hours but CT scan did not show any abnormality. His postoperative course was uneventful. On follow-up after 6 months, he was doing well and his right eye vision shown improvement. Case 2A 28-year-old man presented to us with weight gain, increased size of fingers and toes with thickening, numbness of both hands and palpitation for 3 years. He also had decreased libido. Examination revealed classical acromegalic features. Rest of the neurological examination was normal. Routine biochemical and hematological parameters were normal. Serum growth hormone level was 100 ng/ml. CT scan revealed an iso to hyperdense mass in the sella, which enhanced on contrast administration. He was operated via sublabial rhinoseptal transsphenoidal approach and tumor decompression was done. While removing the sellar floor on the right side, the cavernous ICA was injured, with profuse bleeding which was controlled with packing. Patient was ventilated for 24 hours. An angiography revealed a CCF, which was embolized using 2 gold valve balloons. A check angiogram showed complete occlusion of the CCF. After 1 week, there was recurrence of CCF along with the development of large false aneurysm due to deflation of one of the balloons (Figure 3). This was occluded using GDC coils. A left carotid angiogram with cross-compression showed good cross-circulation. He had a stormy post-operative period. He developed left hemiplegia and right complete ophthalmoplegia from which he was recovering at the time of discharge. At follow-up after 3 months he was independent and had only minimal deficits. Discussion Although transsphenoidal surgery is a safe and effective procedure with excellent results, life-threatening complications may occasionally result with this approach. Hemorrhage from the carotid artery is a potentially fatal complication. Although considered a rare occurrence, this complication has been experienced by 12% of pituitary surgeons in a recent national survey.2 Raymond et al,3 encountered arterial injuries during transsphenoidal surgery in 1% of their cases which was the cause of significant morbidity (24%) and mortality (14%). Carotid cavernous fistula, false aneurysm and carotid occlusion have all been reported.3-11 The anatomy of the pituitary region and its fossa is extremely variable. Renn and Rhoton12 emphasized the great variation in distance between the carotid arteries within the sella and supraclinoid region, being as small as 4 mm in 10-12% of cases. The carotids were exposed in the sphenoid sinus with no bony coverings in 4% of the cases, and were sometimes covered only by mucosa. Variations in the arterial anatomy predispose to vascular injury. On the venous side, an anterior intercavernous sinus was found in 76%, and a posterior sinus in 32% of cases. A large anterior sinus can be particularly hazardous. Intrasellar persistent trigeminal artery and other anomalies have also been described.13 Considering these factors, the reported incidence of carotid false aneurysm is surprisingly low. Both Jakubowski and Kendall14 and Nakstad and Skalpe15 advocated routine angiography in the preoperative assessment of patients prior to transsphenoidal surgery because of the variable anatomy and the risk of aneurysm formation. Richmond et al16 however, suggest a more selective use of angiography for those patients in whom CT suggests a variable anatomy. These cases emphasize the need for a clear understanding of the regional anatomical variations by surgeons undertaking transsphenoidal surgery. In most of the patients, profuse bleeding at surgery was controlled with nasal and sphenoid packing, followed by a cerebral angiography and subsequent definitive treatment. Packing may suffice but if it does not, an otherwise treatable complication may well become a disaster. Several authors have described delayed disasters such as massive epistaxis and possible death.3,4,6,9 Raymond et al,3 recommend balloon occlusion of the carotid artery for carotid cavernous fistulas, carotid stenosis, and carotid false aneurysms, if the patient can tolerate carotid test occlusion and the anatomy of the circle of Willis is satisfactory. If a patient fails the test occlusion (either by clinical examination or cerebral blood flow imaging testing), he is a candidate for some form of surgical bypass, provided epistaxis is well controlled and the hemodynamic condition is stable. They also recommend that sudden arterial bleeding should be controlled by packing. An immediate postoperative angiography should be performed in all patients. If postoperative angiogarphic findings are normal, a repeat study is recommended after the nasal pack is removed and before the patient is discharged. Fukushima and Maroon17 recently described a new technique in 4 cases of carotid injury by using Teflon mesh and methyl methacrylate to form an external, artificial wall over the laceration and the carotid artery. Angiography and neurointerventional techniques are not universally done, but are strongly recommended prior to or along with pack removal. As emphasized by others, subsequent follow-up angiography is essential, even after successful control of carotid hemorrhage. With current neurointerventional techniques, these complications can be handled in endovascular techniques. Otherwise, more aggressive surgical approaches may be required. Acknowledgement The authors wish to thank Prof. K. Mohan Das, Director, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, India, for his kind permission to publish this manuscript. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03022f2.jpg] [ni03022f3.jpg] [ni03022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}