 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 51, No. 1, Jan-Mar, 2003, pp. 87-88 Case Report Gluteal abscess: A manifestation of Pott's spine R. Kumar, A. Chandra* Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical
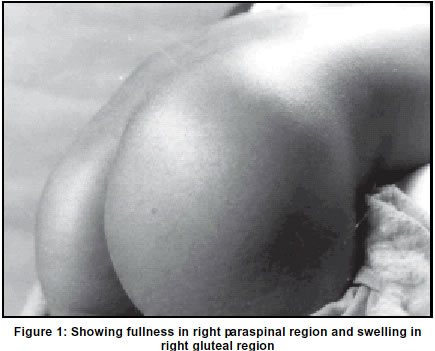
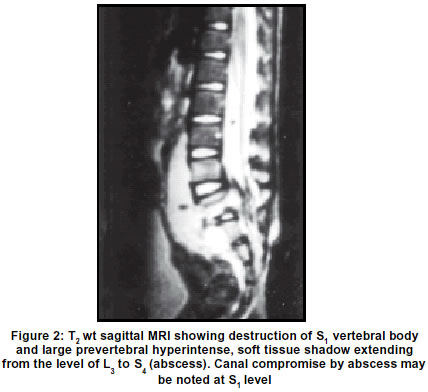
Sciences, Lucknow-226014, India. Accepted on 03.09.2001. Code Number: ni03024 A 3-year-old girl presented with features suggestive of compression of cauda equina. In addition, she had soft, fluctuant gluteal swelling, which on aspiration yielded pus, positive for acid-fast bacilli on staining and culture. She showed significant clinicoradiological improvement following aspiration of pus and antitubercular treatment. Rare manifestations of cold abscess in the spine are discussed. Key Words: Pott's spine, Cold abscess, Tuberculosis spine, Gluteal abscess. Vertebral tuberculosis is the commonest form of the skeletal tuberculosis.1-4 It is most common during the first three decades, though the disease may occur at any age between 1 to 80 years.1 Most commonly, it affects the thoracic and thoraco-lumbar spine.1,2,4 TB of cervical spine is most common in children.1 The clinical manifestations of Pott's spine are protean. The patient of Pott's spine under discussion was admitted with an extremely uncommon clinical finding of gluteal abscess. Case Report A 3-year-old female child was admitted with complaints of low grade fever off and on for 6 months, difficulty in walking for 3.5 months and pain at the back and a right gluteal swelling for 15 days. Neurological examination revealed grade 4/5 paraparesis. Bilateral knee jerks were brisk with bilateral absent ankle jerks. Bilateral plantars were equivocal. There was no sensory deficit. Local examination of the spine showed dorsolumbar scoliosis with convexity to right, tenderness at lumbosacral junction and an ill-defined swelling in the right paraspinal region, more prominent in the right gluteal region (Figure 1). Plain radiography of the lumbosacral spine showed collapse of S1 vertebra with scoliosis. Magnetic resonance imaging (MRI) of the thoracolumbar region with saggital T1 weighted, T2 weighted and proton density image with axial T1 weighted images showed destruction of the S1 vertebra and focal canal compression by soft tissue at S1 level. There was a large pre and paravertebral loculated soft tissue shadow which was hypointense on T1 weighted and hyperintense on T2 weighted images (Figure 2). Prevertebral soft tissue shadow extended form L3 to S4 vertebrae. It also extended into the spinal canal. Hematological examination revealed leucocytosis with raised ESR. Considering the clinicoradiological diagnosis of Pott's spine, the child was taken up for surgical decompression. A needle was introduced at the point of maximum swelling, which yielded 35 ml of pus. This pus was positive for acid-fast staining and culture. She was put on antitubercular treatment, and she showed significant improvement at 2 month's follow-up. She walked independently at 6.5 months follow-up. A plain skiagram of the lumbo-sacral spine demonstrated good healing and callus formation at the S1 vertebral level. Discussion The prevalence of tuberculosis is around 30 million globally and approximately one-third of the cases are found in India.2 1 to 3% of the 10 million have involvement of bones and joints.1,2 Vertebral tuberculosis is the commonest form of skeletal tuberculosis comprising about 50-70% of all bone and joint tuberculosis.1,2 Any osteoarticular tubercular lesion is the result of hematogenous dissemination from a primarily infected visceral focus, an established common route of spread being Batson's prevertebral venous plexus.1,2,4 The youth are more vulnerable to the disease but it can occur at any age. Acute presentations are uncommon.1 The usual presenting symptom of skeletal tuberculosis is pain.5 Constitutional symptoms such as weight loss, lassitude, loss of appetite and evening rise of temperature are common.1 There may be stiffness and painful, restricted joint movements in all planes. Severe spasm of adjacent muscles is common. A cold abscess may occur in long-standing cases which tracks it's way through the intermuscular planes. A deformity in the spine can present as kyphosis, along with local tenderness.1,2 Tuli reported clinically palpable cold abscess in 20% cases and radiologically visible perivertebral abscess in 21% cases of Pott's spine.1 Tuberculosis of the spine has the following distribution_thoracic 42%, lumbar 26%, thoracolumbar and cervical each 12%, cervicodorsal 5% and lumbosacral 3%.1 The lesion in the spine is most often paradiscal in location with destruction of the disc, reduction of the disc space and concomitant destruction of the vertebral bodies on either side of disc space.1,2,6 The destruction occurs in the anterior aspect of the vertebral body and extends behind the anterior longitudinal ligament. It may remain confined to the centrum of the vertebrae, resulting in a concentric collapse. Lastly, posterior element disease can occur in the posterior neural arch. The disease can involve the vertebral bodies at two or three different sites and these are referred to as "Skipped lesions", which occur in about 7% cases. 12% patients have associated involvement of other bones and joints (including spine).1,6 Because of the subtle nature of the symptoms, diagnosis is often missed until the disease is advanced. Delay in diagnosis can be catastrophic in vertebral tuberculosis. The extension of disease process can cause compression of the spinal cord leading to severe and irreversible neurologic sequelae including paraplegia.3 A lumbar cold abscess can spread along the aorta and its branches to present at the: (a) ischiorectal fossa, (b) in the buttock under the gluteus maximus, as in our case, because of the large size of the abscess in the prevertebral and paravertebral region it could rupture and track along the branches of aorta to manifest as a gluteal abscess, (c) along the psoas sheath or (d) in the lumbo-dorsal region (Petit's triangle). It can also track down along the femoral or obturator artery and present on the medial side of the thigh, femoral triangle, popliteal fossa or on the medial side of the tendo-achilles.2 Dinc H7 also reports a case of multilocular pelvic and gluteal tuberculous abscess, which was treated with CT guided percutaneous drainage. Thus the initial presentation of a cold abscess can be far away from the site of lesion. References
Copyright 2003 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni03024f2.jpg] [ni03024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}